


Canine Spinal Empyema and Meningitis
The patient
A 4-year-7-month-old male neutered dog (Chihuahua mix) presented with a 1-month history of progressive neck pain, ataxia, and tetraparesis. Additionally, the dog had become hyporexic over the last week and hypodipsic in the previous few days. The neurological exam was compatible with a C1-T2 myelopathy. The dog underwent a cervical vertebral column MRI using the Hallmarq 2nd generation 1.5T unit (see Fig 1).
The imaging results
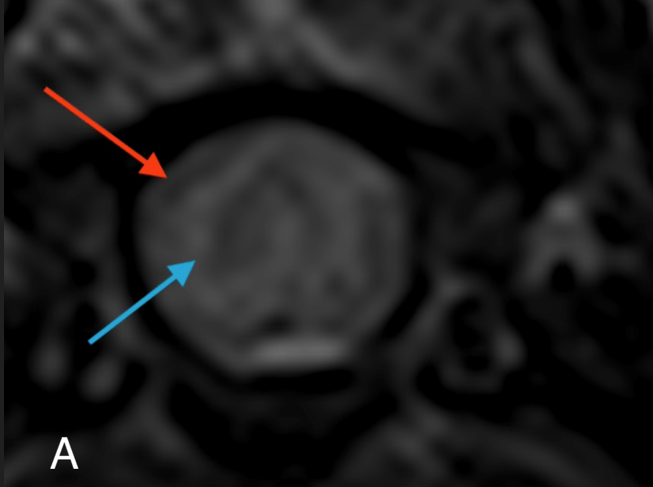
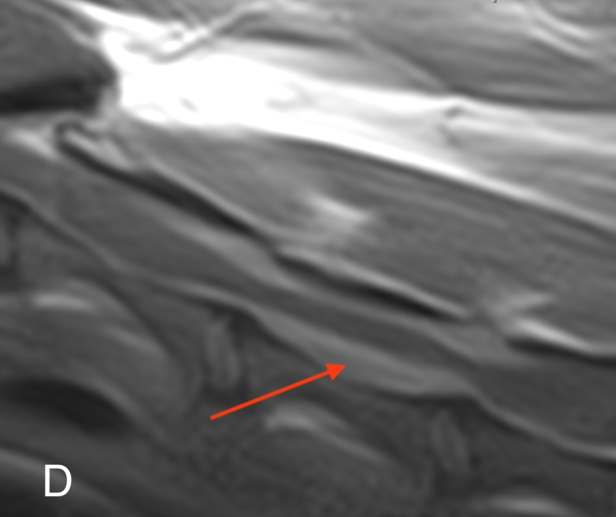
There is a poorly defined and irregular intramedullary T2W and STIR hyperintensity extending from C3 to C5 with a loss of the T2W hyperintense circumferential subarachnoid signal in this region (A). Cranial to this lesion there is dilation of the central canal over C2-C3. There is also an ill-defined and irregular extradural lesion seen predominantly on the right side over C3-C5 but also dorsal and ventral to the cord which is T2W hypointense to the cord and strongly contrast enhances in both a heterogeneous and a ring-like manner (B and D).

This lesion is associated with moderate cord compression. The adjacent meninges also strongly enhance (C and D). There is moderate enlargement of the mandibular and medial retropharyngeal lymph nodes.

The imaging study is compatible with empyema and meningitis which in this case was associated with a positive titer for the fungal organism, Coccidioides. Without cytology and culture of the epidural lesion, this presumption cannot be confirmed with the imaging characteristics also being compatible with lymphoma and meningeal neoplasia such as histiocytic sarcoma, meningioma, and metastatic carcinoma.
The most valuable MRI sequence for this case
The post-contrast images in this case highlight the extent of the meningeal involvement and the extradural compressive lesion.
Disease overview
Spinal epidural empyema is defined as an extensive accumulation of purulent material in the epidural space of the vertebral canal. Migrating foreign bodies such as grass seeds, extension from adjacent infected tissues, penetrating injuries, or haematogenous spread from a distant site are potential sources of the infection, which is most commonly bacterial but can be fungal as in this case. Given the proximity of the infection, vertebral osteomyelitis or discospondylitis are often seen in association with spinal epidural empyema although were not seen in this case. Clinical signs are likely a consequence of a combination of meningeal inflammation, spinal cord compression, and possible vascular compromise of the spinal cord related to the epidural fluid accumulation. Characteristic clinical signs include pyrexia, acute progressive spinal hyperaesthesia, and progressive myelopathy.
Haematology reveals an inflammatory leucogram. Blood cultures can be positive, with Staphylococcus and Streptococcus species commonly isolated. Radiography may reveal associated vertebral physitis or discospondylitis. Diagnosis is aided by myelography, CT, or MRI, with the identification of extradural compression that extends over multiple spinal cord segments. MRI is most sensitive for assessment of the severity and extent of changes associated with infection of the paraspinal muscles and other soft tissue structures. Cross-sectional imaging can further help to guide surgical therapy if indicated.
The recommended treatment plan
Effective treatment requires rapid institution of an appropriate antibiotic or anti-fungal therapy (broad spectrum pending culture results) and appropriate analgesia. Antibiotic administration should be intravenous initially before transitioning to oral medication. Traditionally, surgery has been considered the treatment of choice to allow drainage of infected material, direct organism culture, and spinal cord decompression. More recent reports suggest that medical management without surgical decompression may be sufficient, particularly in cases with minimal to no spinal cord compression, mild neurological deficits, or severe lesion extension over a long region of the vertebral canal. Therefore, the main benefit of surgical management may be the opportunity to obtain samples for organism culture and antimicrobial sensitivity.
Dogs and cats with spinal epidural empyema may have a good outcome when treated promptly, with appropriate long-term antibiotic therapy ideally based on culture and sensitivity.
Thanks to Dr. Cody Alcot DACVIM, owner of Tucson Veterinary Specialists, AZ, for providing this case study.
References
- Blanco C, Moral M, Minguez JJ, Lorenzo V. Clinical Presentation, MRI Characteristics, and Outcome of Conservative or Surgical Management of Spinal Epidural Empyema in 30 Dogs. Animals (Basel). 2022 Dec 17;12(24):3573
- Laws EJ, Sánchez L, Beltran E, Domínguez E, Ekiri AB, Brocal J, De Risio L. Multicenter Study of Clinical Presentation, Treatment, and Outcome in 41 Dogs With Spinal Epidural Empyema. Front Vet Sci. 2022 Mar 7;9:813316
