

In this case study, we take an in depth look at a long medial collateral ligament injury of the fetlock joint with associated injury of the medial condyle of the third tarsal bone. In addition to detail obtained from ultrasonographic and radiographic findings, standing MRI enabled a comprehensive assessment of the pathology, adding to the information and allowing a more informed assessment of prognosis.
History
The horse was admitted for investigation of left hindlimb lameness with generalized swelling of the distal limb. The horse had been treated with antibiotics and NSAIDs. The swelling gradually became more localized to the fetlock joint and synoviocentesis ruled out sepsis of the joint. A palmar digital nerve block, abaxial sesamoid nerve block and intra-articular anesthesia of the fetlock joint were negative.
Ultrasonographic & Radiographic Findings
Ultrasonographic examination revealed disruption of the long medial collateral ligament of the fetlock and irregular contours of the bony surface of the medial condyle of the third metatarsal bone at the site of the short medial collateral ligament of the coffin joint.
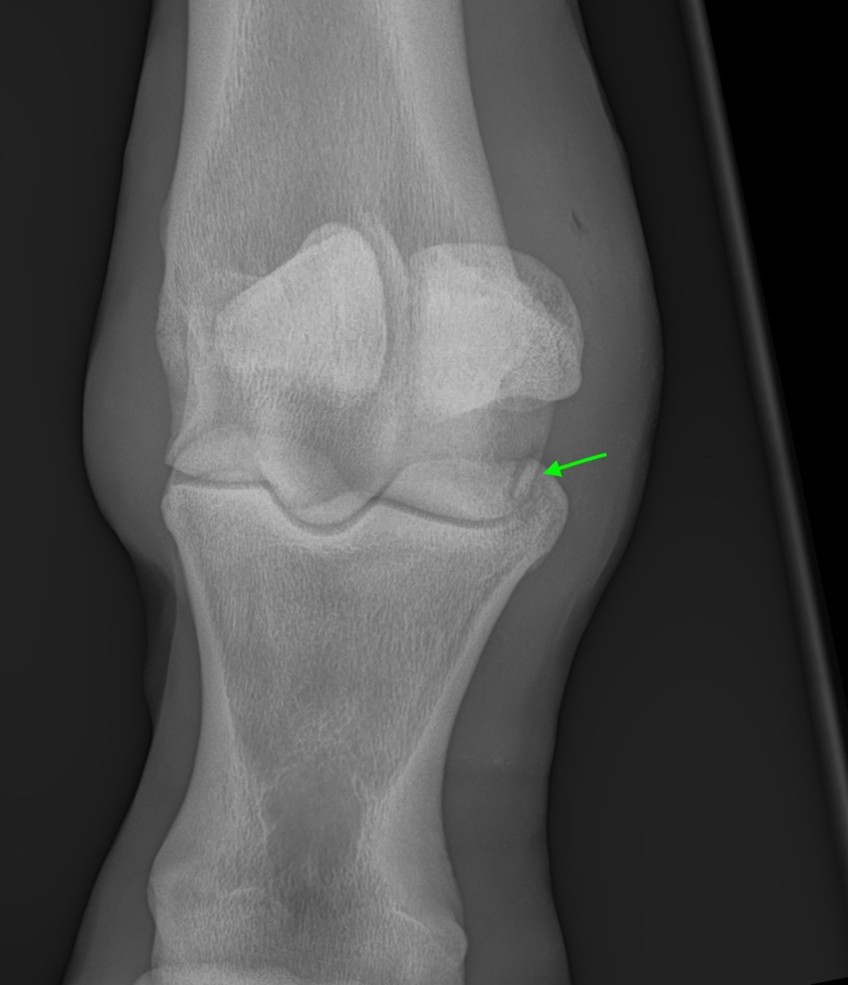
Radiographic examination of the fetlock revealed a curved radiolucent line at the plantar aspect of the medial condyle of the third metatarsal bone with small bony fragments.
MRI Findings
The horse underwent standing MRI of the left hind fetlock joint. Soft tissue swelling was present along the medial aspect of the distal metatarsal region originating close to the origin of the long collateral ligament of the fetlock joint and extending distally to the medial aspect of the fetlock.
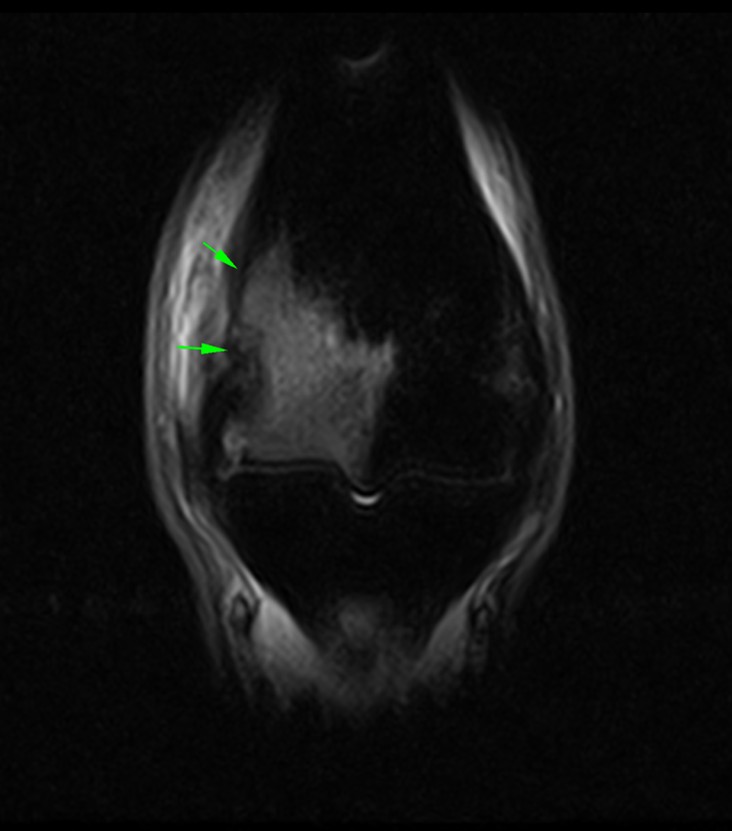
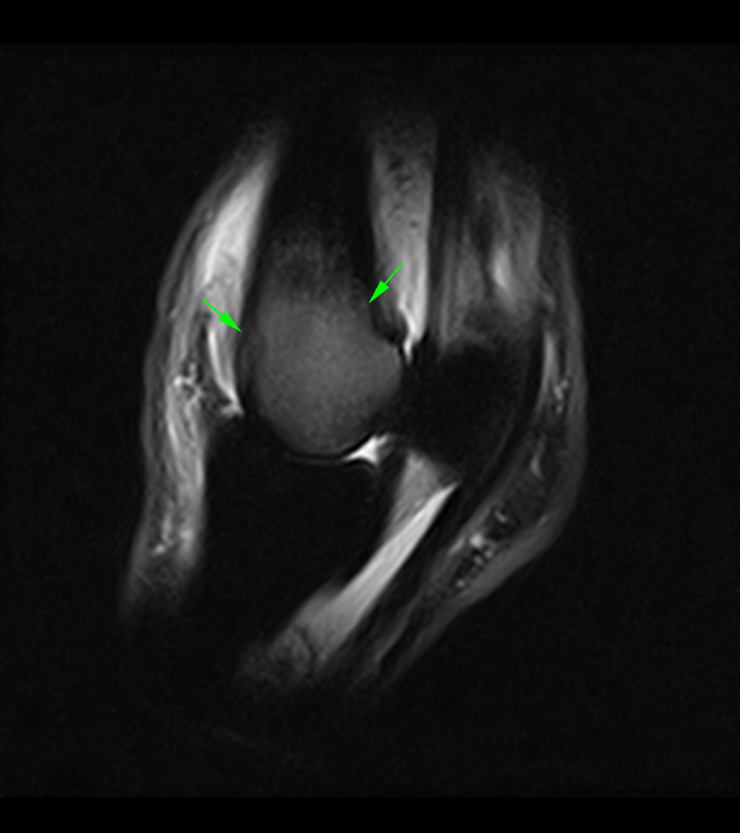
There was marked enlargement and disruption of the long medial collateral ligament of the fetlock joint with diffuse increased signal intensity on T2W and STIR sequences (Figure 2).
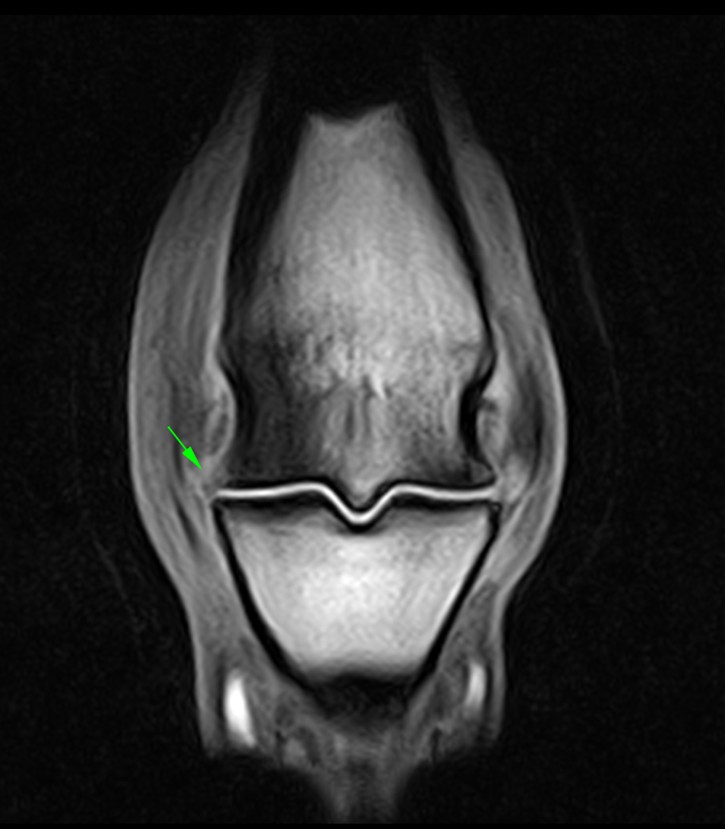
There was marked increased STIR signal intensity and T2*W fat water cancellation artefact (bone marrow fluid signal) at the medial condyle of the third metatarsal bone extending proximally above the physeal scar and axially towards the sagittal ridge (Figure 3).
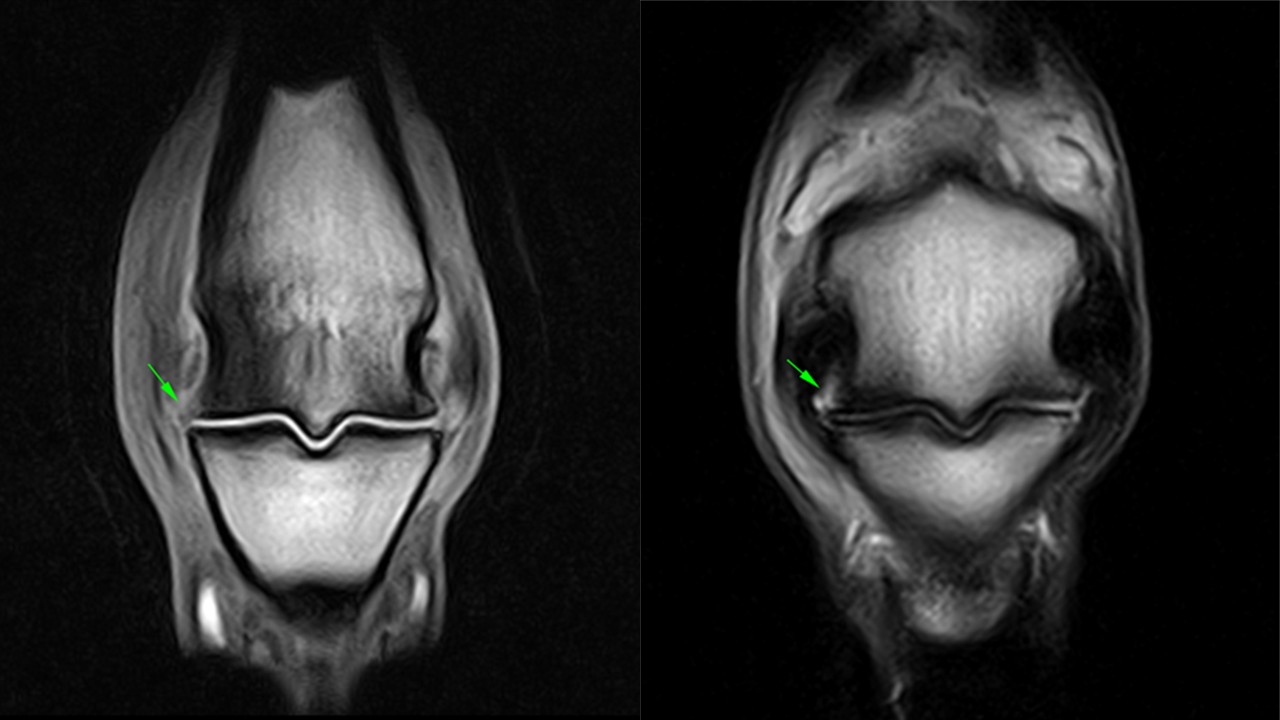
Loss of definition of the medial articular margin of the third metatarsal bone was visible, with apparent loss of bone from the articular margin extending a very short distance proximally from the medial articular margin. There was also pooling of synovial fluid between the disrupted margin of the bone and the short medial collateral ligament of the joint (Figure 4).
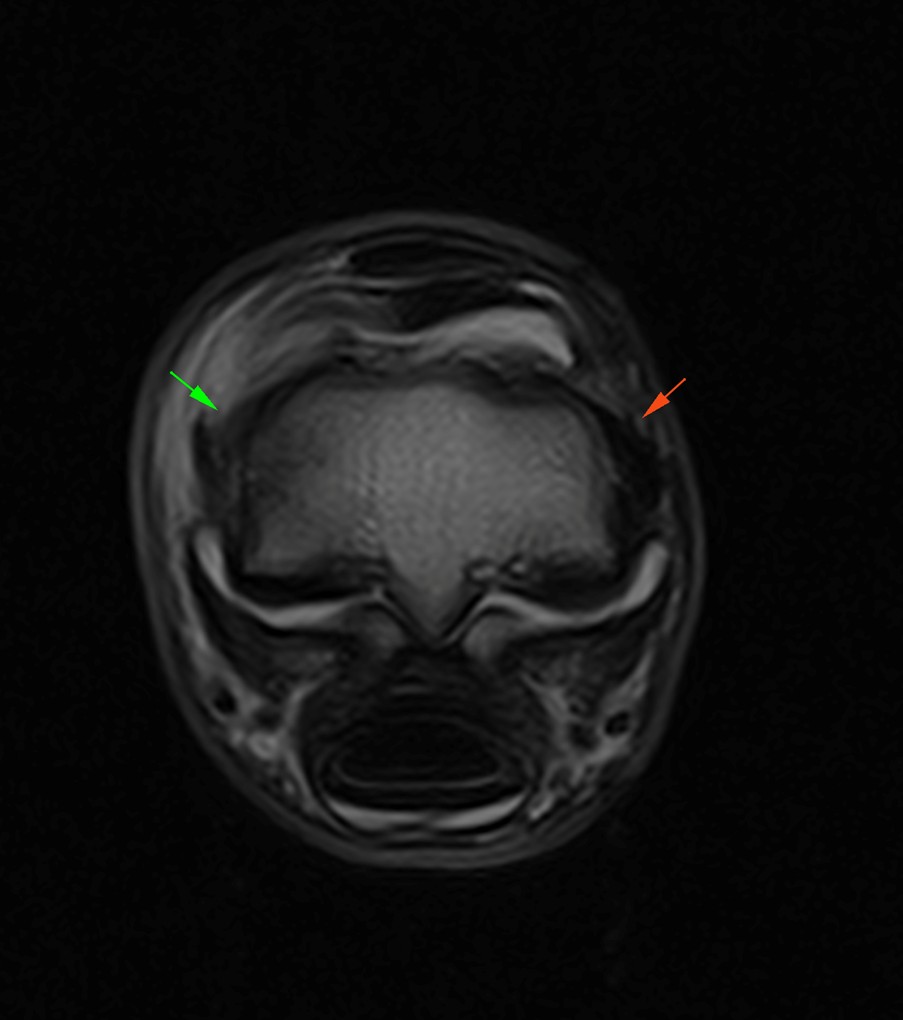
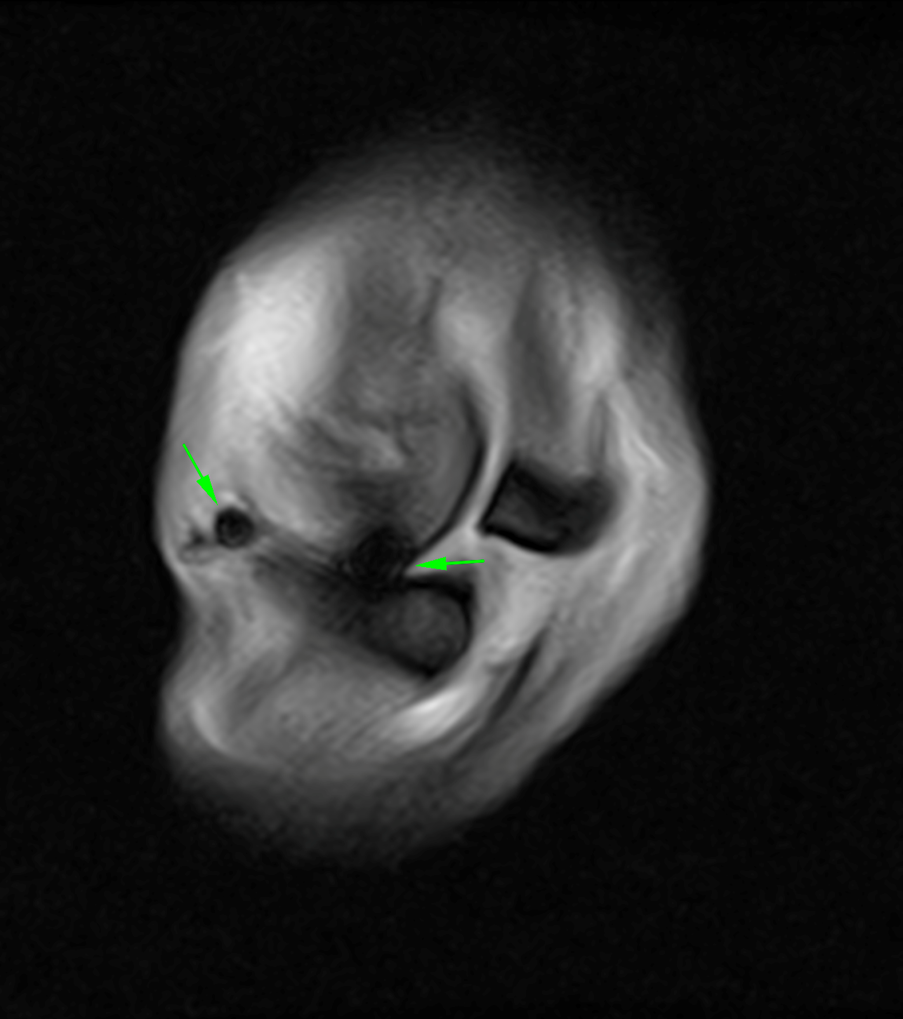
Magnetic susceptibility artefacts within the medial joint space were most consistent with focal hemorrhage (Figure 5). The fetlock joint was distended with joint effusion and wispy intra-articular tissue.
Figures 3a and 3b: Frontal and Sagittal STIR FSE iNAV sequences showing diffuse bone oedema throughout the trabecular bone of the medial condyle of the third metatarsal bone.
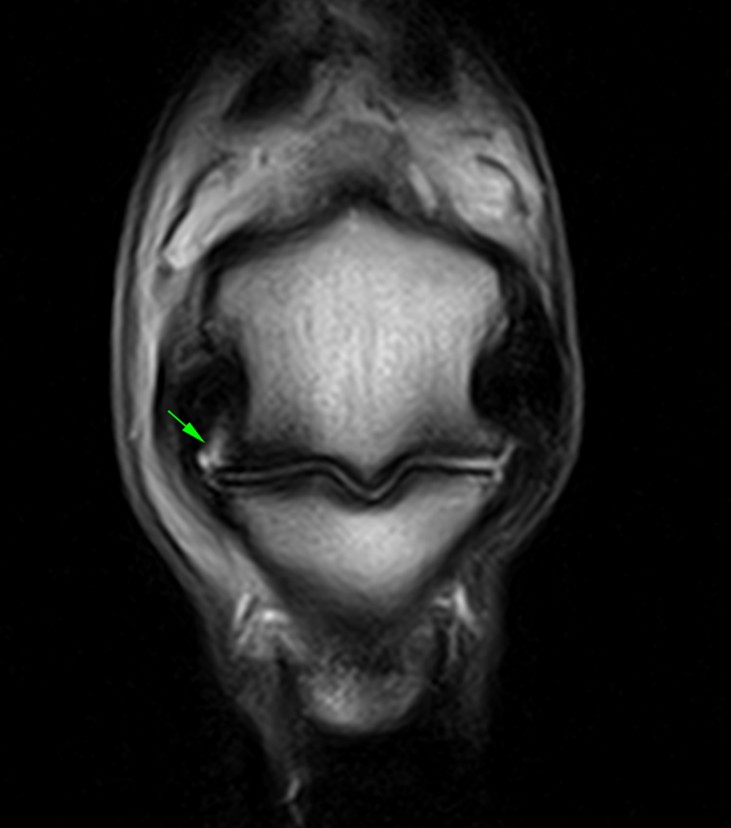
Figures 4a and 4b: Frontal T1W 3D and T2E FSE iNAV sequences showing loss of clear definition to the medial articular margin of the third metatarsal bone with pooling of synovial fluid between the disrupted bony margin and the axial margin of the short medial collateral ligament of the fetlock joint.
Conclusion
There was generalized active disruption of the long medial collateral ligament of the fetlock joint and disruption of the bony margin of the medial condyle of the third metatarsal bone. In addition, extensive bone edema was present throughout the trabecular bone of the medial condyle, extending proximally along the medial aspect of the bone. This bone edema was considered likely to represent inflammation and potentially hemorrhage within the trabecular bone. There was also evidence of hemorrhage within the soft tissues along the medial aspect of the joint.
MRI identified several abnormalities, both soft tissue and osseous injuries of the fetlock and allowed differentiation and characterisation of these lesions. This provided a more comprehensive assessment of the pathology, adding to the information obtained from the ultrasonographic and radiographic findings and allowing a more informed assessment of prognosis.
Prognosis
In this specific the case of long medial collateral ligament injury of the fetlock joint with associated injury of the medial condyle of the third tarsal bone, the prognosis for the horse returning to its previous level of athletic performance was considered poor. Although some improvement in the degree of lameness may occur over time, a degree of lameness may persist. Given the disruption of the articular surface and the likely joint instability associated with disruption of the long medial collateral ligament, osteoarthritic changes may develop over time.
To learn more about the use of Standing Equine MRI in equine lameness diagnosis, you can access our full guide here…
With thanks to Dr Becky Jones and Anthony Hall, B&W Equine Vets, UK for sharing this case study with us.
