


The Patient
In a case of non-traumatic feline tail paralysis, a 10-year-old male-neutered Siamese mix cat presented for an acute progressive onset of a flaccid tail. In addition, he had progressive pelvic limb weakness with ataxia. However, there was no history of trauma or ongoing health issues. On examination, the cat exhibited a normal level of awareness and behavior with normal cranial nerve function. The cat was ambulatory, with mild paraparesis and moderate spinal ataxia affecting both pelvic limbs. The pelvic limbs exhibited a reduced level of proprioception. The tail was plegic and flaccid. A suspected multifocal neurological disease was localized to the T3-caudal spinal segments.
The cat underwent a caudal lumbar vertebral column MRI using Hallmarq’s 1.5T small animal, zero-helium MRI machine (see Figs 1 and 2).
The Imaging Results
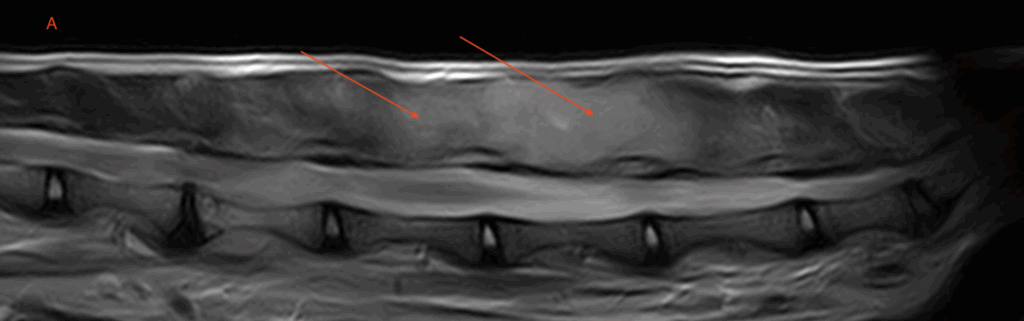
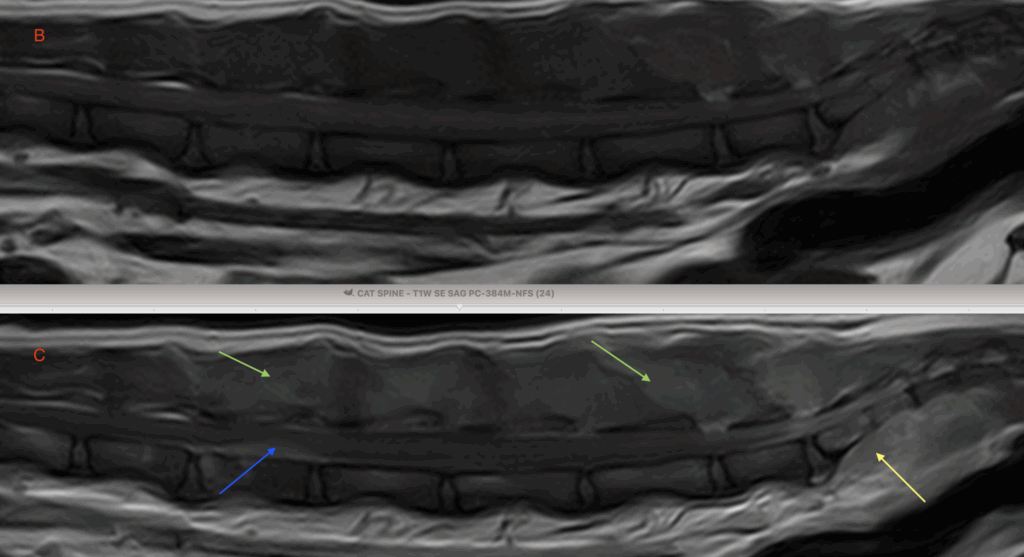
Fig 1 (A) T2W sagittal lumbar vertebral column. There are broad regions of ill-defined and irregular increased signal intensity associated with much of the epaxial musculature, spanning from the level of L2-3 through to the level of the sacrum (red arrows). The regions of abnormal signal intensity are also appreciably swollen compared to normal muscle tissue. These regions are isointense to normal musculature on T1-weighted sequences (B) but undergo moderate contrast-enhancement (C) (green arrows). Additional regions of increased signal on T2W images that demonstrate similar enhancement are noted ventral to the sacrum (yellow arrows). A lesion within the vertebral canal is noted over the level of the L3 vertebral body on these images (blue arrow).
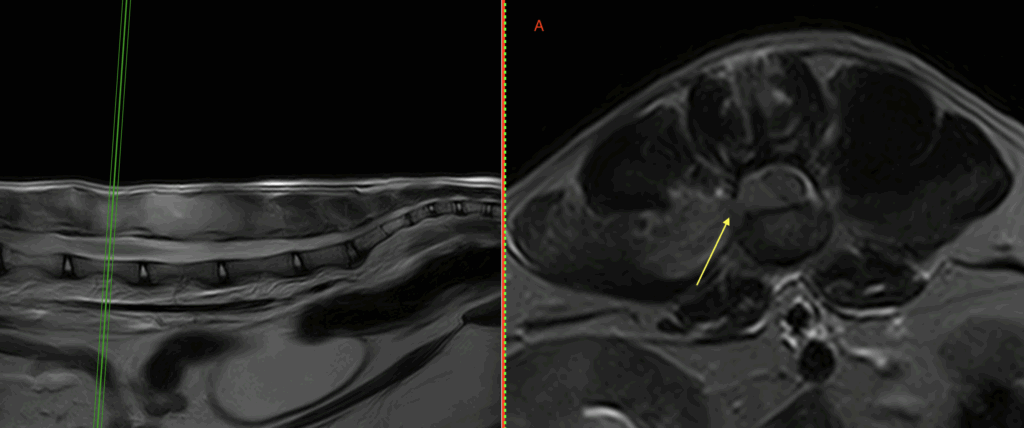
Fig 2. (A) T2W, (B) T1W pre-contrast and (C) T1W post-contrast transverse images at the level of L4. Some of this T2W hyperintense and abnormally enhancing tissue seen in Figure 1 extends through the right intervertebral foramen at L3-4 (yellow arrow), occupying the right ventral aspect of the spinal canal and causing moderate displacement and mild compression of the spinal cord at that level (Red arrow).
A lumbar CSF tap revealed a mild neutrophilic cell elevation (pleocytosis).
A fine needle aspirate of the epaxial musculature using the location of the lesions identified on the MRI revealed a moderate to large round cell infiltrate compatible with an intermediate to larger cell type lymphoma.
Disease Overview
- Lymphoma of the nervous system accounts for no more than 13% of all lymphomas, most commonly being part of a multicentric neoplastic disease.
- Lymphoma accounts for the most common neoplasm of the spinal cord and the second most common neoplasm of the brain in cats.
- Primary CNS lymphoma accounts for <3% of all primary brain and spinal cord tumors of cats [1].
- Spinal cord lymphomas are typically characterized as epidural masses involving the extradural adipose tissue of the thoracic and lumbosacral segments.
- Intradural or intraparenchymal lymphomas can also occur, especially in cases of spinal cord involvement secondary to multisystemic lymphoma.
- Lymphomas of the peripheral nervous system have been reported uncommonly in cats but can occur concomitantly with CNS lymphoma, as suspected in this case.
- Widespread infiltration of neoplastic lymphocytes within nerve roots or nerves with or without CNS involvement is referred to as diffuse neurolymphomatosis [2].
A recent study has described the clinical and MRI features of spinal lymphoma in 27 cats [3]. The most frequent neurological signs were rapidly progressive paraparesis (62.9%) or paraplegia (22.2%). A bimodal age distribution was found with 40.7% of cats aged ≤2.5 years (63.6% of them FeLV positive), and 44.4% of cats aged ≥8 years (16.7% of them FeLV positive). Spinal lymphoma generally appeared on MRI as an ill-defined epidural focal lesion with moderate to severe spinal cord compression, expanding more than one vertebral body. MRI lesions were typically hyperintense on T2-weighted sequences and isointense on T1-weighted sequences.
The degree and pattern of contrast enhancement were variable in this study. Other morphological patterns included paravertebral masses with extension into the vertebral canal and lesions centered in the spinal nerve roots, as seen in this case. Confirmation of spinal lymphoma was performed by CSF analysis in 4/27 (14.8%) of cases, by FNA in 6/27 (22.2%) of cases, and by surgical biopsy in 10/27 (37%) of cases. Tissue sampling guided by MR imaging findings remains necessary for definitive diagnosis of non-traumatic feline tail paralysis in many instances, as with the cat described in this report.
References
- [1] Rissi DR, McHale BJ, Miller AD. Primary nervous system lymphoma in cats. J Vet Diagn Invest. (2022) 34:712–7. 10.1177/1040638722109028
- [2] Mandara MT, Domini A, Giglia G. Feline lymphoma of the nervous system. Immunophenotype and anatomical patterns in 24 cases. Front Vet Sci. 2022 Sep 8;9:959466.
- [3] Lorenzo V, Ribeiro J, Bernardini M, Mínguez JJ, Moral M, Blanco C, Loncarica T, Gamito A and Pumarola M (2022) Clinical and magnetic resonance imaging features, and pathological findings of spinal lymphoma in 27 cats. Front. Vet. Sci. 9:980414
With thanks to Dr. Adam Moeser and team at Wisconsin Veterinary Neurology & Surgical Center for sharing this case study with us.
