


Bilateral chondral lesions of the distal interphalangeal joint in a warmblood
History
An 18-year-old Warmblood gelding was presented with a right forelimb lameness of chronic duration. The horse had already received intra-articular medication of steroids and hyaluronic acid to both forelimb distal interphalangeal (DIP) joints on multiple occasions in the few years prior to presentation.
Clinical examination
There was mild distension of the dorsoproximal recess of the DIP join on both left and right forelimbs. Initially a 2/5 (AAEP lameness grade) right forelimb lameness was observed which resolved after a RF abaxial sesamoid nerve block. Lameness then switched and a 1/5 (AAEP lameness grade) was observed in the left forelimb which resolved after a LF abaxial sesamoid nerve block. The horse then remained sound.
Radiographic findings
Mild osteophyte formation at the dorsoproximal articular margin of the distal phalanx was evident bilaterally. No other abnormalities were noted (Fig. 1).
MRI findings
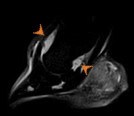
On the right forelimb, there was focal low signal in T1 and T2*-weighted high-resolution sequences at the lateral aspect of the cartilage layers of the distal interphalangeal joint indicative of full thickness erosion (Fig. 2). There was no associated subchondral bone remodelling or inflammatory changes. There was moderate narrowing of the interarticular space at the lateral aspect of the DIP joint. Hyperintense signal in the STIR images indicated moderate distension of the dorsoproximal and palmaroproximal recesses of the DIP joint consistent with the clinical examination (Fig. 3). Mild chronic remodelling of the navicular bone was also noted with similar findings evident in the left forelimb DIP joint.






Diagnosis
Bilateral chondral lesions of the palmaro-lateral aspect of the distal interphalangeal joint with associated secondary synovitis.
Treatment and prognosis
Arthroscopic exploration with a view to debridement of the lesions was advised, but this treatment option was declined by the owner on the basis of the age of the horse and subsequent expected use. The horse was treated with intra-articular DIP joint medication (steroids and hyaluronic acid) and intramuscular glycosaminoglycans. The horse returned to work and the condition was managed with regular assessment and DIP joint medication as required.
