

For equine vets, diagnosing pathology of the proximal suspensory can be a challenge as was the case with this particularly tricky patient seen by Donnington Grove Equine Vets. .
Case History
The horse sustained an avulsion fracture of the right forelimb proximal suspensory origin approximately six months prior to referral. Despite a structured rehabilitation programme, lameness persisted and failed to fully resolve
Follow-up radiographic and ultrasonographic assessments were challenging due to the extent of the injury and failed to provide a definitive explanation for the ongoing lameness. Given these limitations, standing equine MRI was performed to obtain a more detailed evaluation of the affected region.
MRI Findings
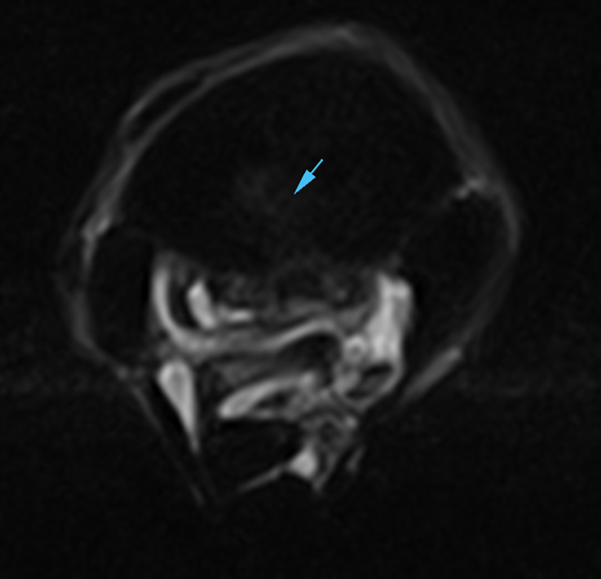
Standing equine MRI of the right proximal metacarpal region revealed marked sclerosis of the proximal metacarpus, and mild, diffuse fluid signal within the palmar cancellous bone of the third metacarpal bone, indicative of bone marrow edema. The avulsion fragment was identified as an approximately triangular-shaped region with associated fluid signal within the suspensory ligament immediately distal to the avulsion site, suggestive of ongoing inflammation.
The interface between the suspensory ligament and the adjacent bone was poorly defined, raising suspicion of adhesion formation. Additionally, there was enlargement of the medial lobe of the suspensory ligament with signal alterations consistent with chronic fibrosis and moderate desmopathy.
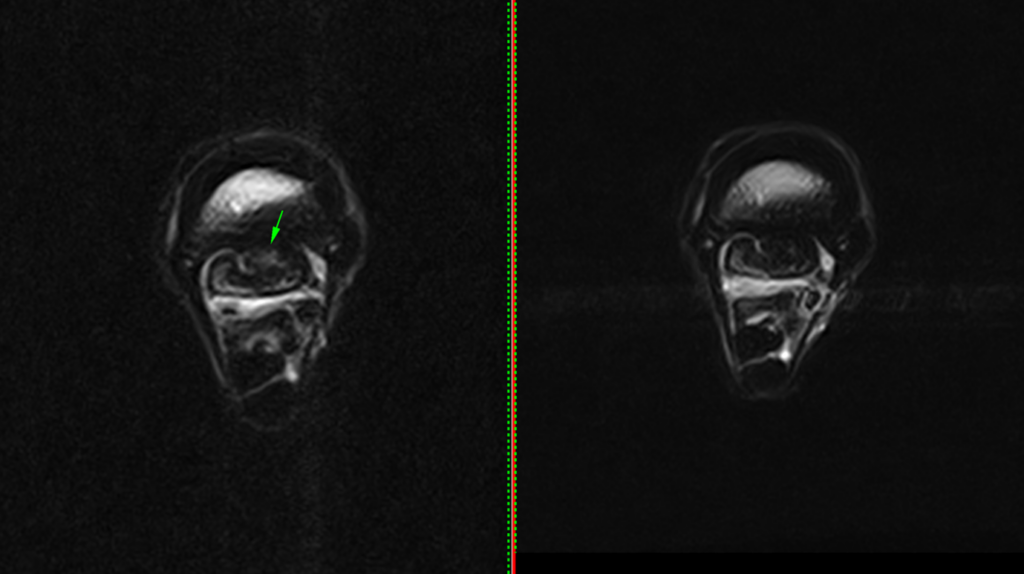
Figures 1A and 1B above: T1 GRE MI transverse scan showing the sclerosis of the proximal metacarpus (green arrows) and avulsion fragment (blue arrow).
Standing MRI provided a more comprehensive evaluation of the injury and its stage of healing. The identification of fluid signal within the suspensory ligament, indicative of ongoing inflammation, was crucial in guiding the subsequent rehabilitation plan—information that could not have been extrapolated from ultrasonography alone. While the avulsion fragment was also visible on radiographs, radiographic imaging does not provide insight into bone marrow edema, which is also indicative of activity of bone injury.

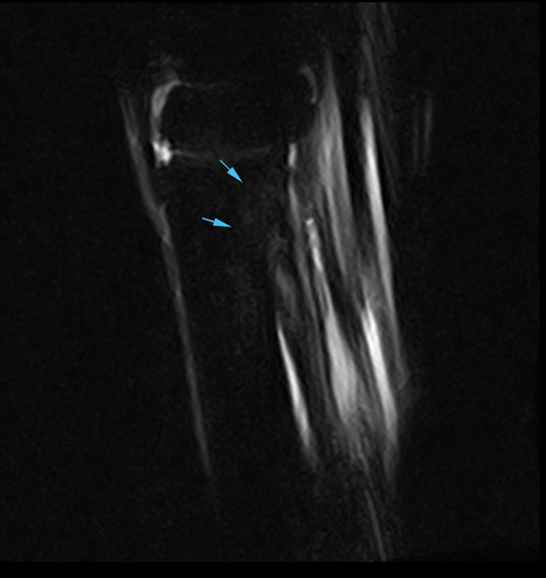
Figures 2 A, B and C above: STIR FSE INAV transverse and sagittal scans showing the mild fluid signal of the third metacarpal bone.
Furthermore, with the implementation of iNAV – Hallmarq’s new motion correction sequence – STIR images were of high diagnostic quality despite increased patient movement. Previously, such motion would likely have resulted in non-diagnostic scans and an inconclusive diagnosis

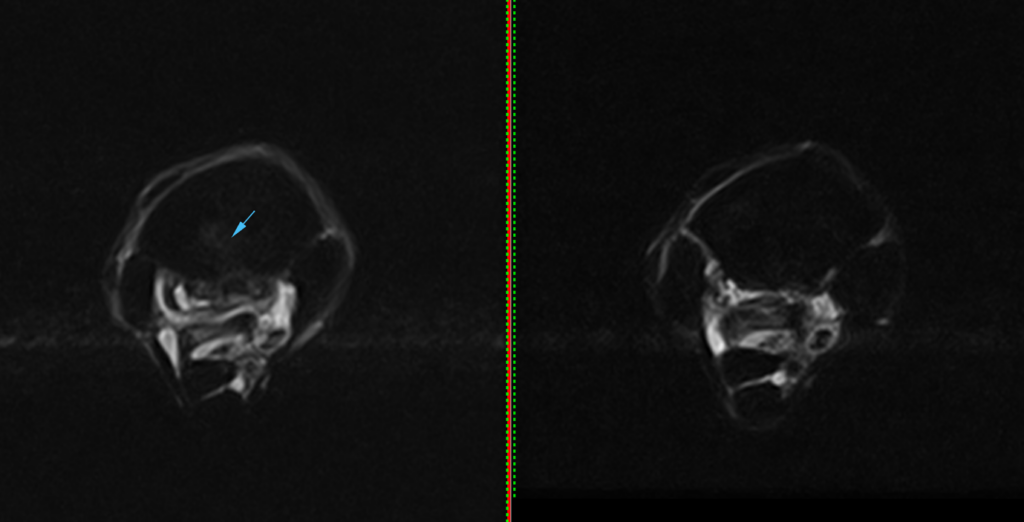
Figures 3A and B above: T1 GRE MI and STIR FSE INAV transverse scans showing the enlargement and signal alterations of the medial lobe of the suspensory ligament indicating chronic fibrosis (green arrows), and the fluid signal consistent of ongoing inflammation (blue arrow).
Conclusion
Diagnosing pathology of the proximal limb remains challenging but advances in MRI software now allow for the acquisition of critical information that complements conventional imaging modalities such as radiography and ultrasonography.
Repeat MRI – Case Study Update
The horse maintained a strict program of only walking exercise and – 3 months after the initial MRI (9 months after the injury) – had a repeat MRI examination to assess the healing process.
Repeat standing equine MRI of the right proximal metacarpal region revealed reduction of the fluid signal within the suspensory ligament just distal to the avulsion fracture indicative of reduced inflammation. The enlargement of the medial lobe of the suspensory ligament and signal alterations are consistent with chronic fibrosis and moderate but less active desmopathy. The mild diffuse increase in STIR signal within the palmar cancellous bone of the proximal third metacarpus has resolved.
Consistent with the assessment 3 months prior, radiographic and ultrasonographic findings continued to have limited value due to the chronic nature of the injury and did not fully correlate with the clinical picture.
A repeat MRI examination, performed 3 months after the previous MRI, allowed for effective monitoring of the healing process. This follow-up MRI demonstrated reduction of the fluid signal within the suspensory ligament and complete resolution of the bone marrow oedema indicative of improvement in the previously detected inflammation. Based on these positive findings, the horse could be gradually reintroduced into exercise following a well-structured rehabilitation program
With thanks to Drs Henry O’Neill and Ethan Yizhen Li, Donnington Grove Equine Vets, UK, for sharing this case with us.
Read more about iNAV for enhanced motion correction.
