

Axial osteitis of the proximal sesamoid bones can be a challenging condition to treat and may – at times – be associated with severe lameness. Serial cross-sectional imaging with CT and MRI is beneficial for monitoring the progression of osteolysis, and to further assist in prognostic formulation. In this case study from Dick Vet Equine Hospital, we look at how complementary scanning enabled a definitive diagnosis for the patient.
History
The horse had a history of left forelimb lameness with a negative response to an abaxial sesamoid nerve block and a positive response to a low-four-point nerve block.
MRI Findings
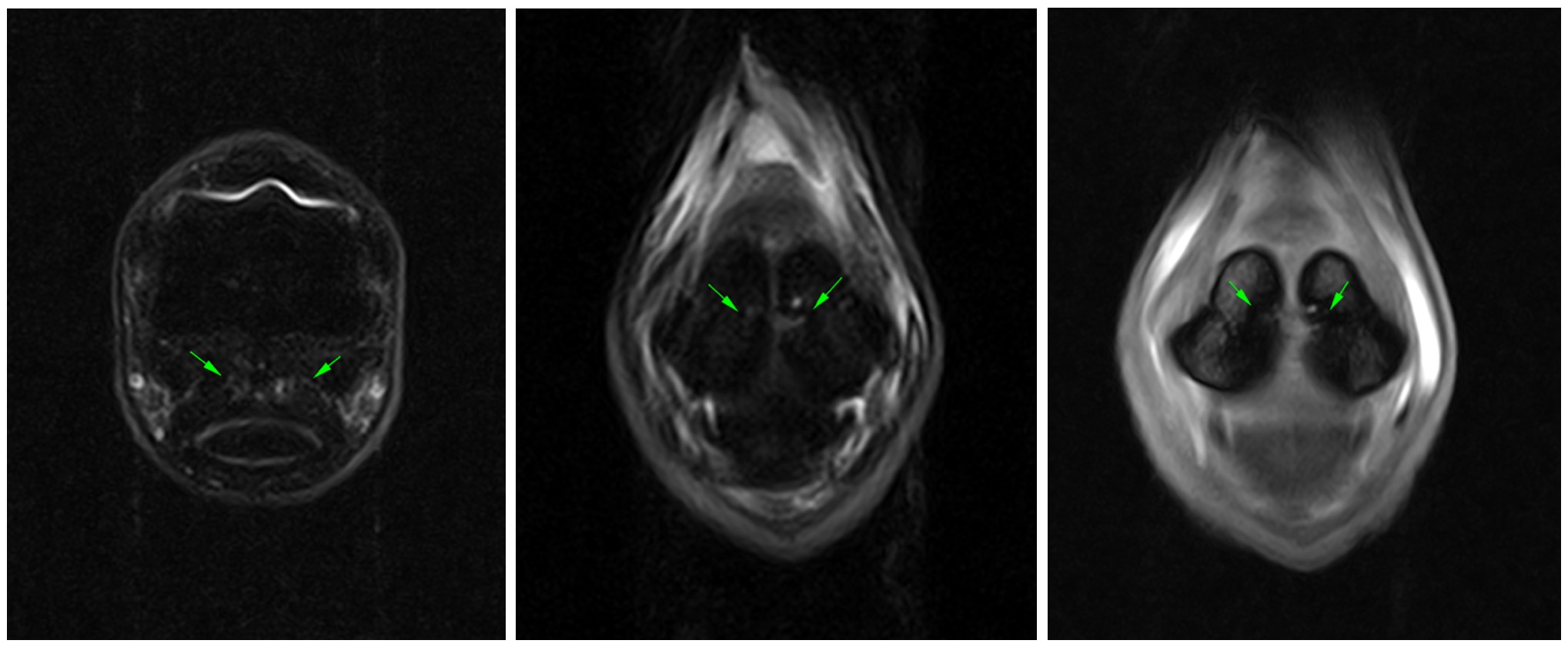
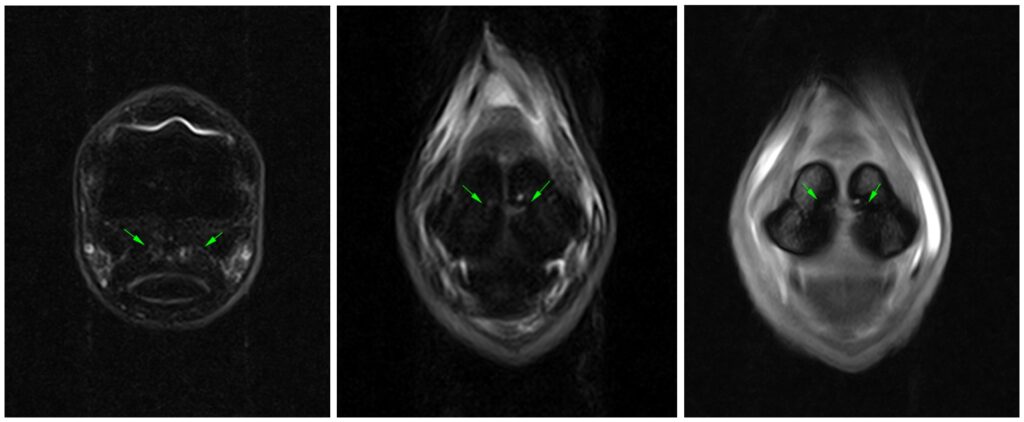
The horse underwent standing MRI of the left front fetlock and proximal metacarpal regions. Scans of the fetlock region, revealed there was moderate distention of the fetlock joint and the dorsoproximal recess of the digital flexor tendon sheath (DFTS). There was reduced T1W and T2W signal intensity at the axial margin of the lateral proximal sesamoid bone associated with a focal increase in STIR signal intensity. There was also mild diffuse increase in STIR signal intensity within the spongiosa of both proximal sesamoid bones, changes that may reflect increased vascularisation or early-stage axial osteitis of the proximal sesamoid bones.
There was a small focal increase in signal intensity on all sequences within the insertion of the medial suspensory branch.
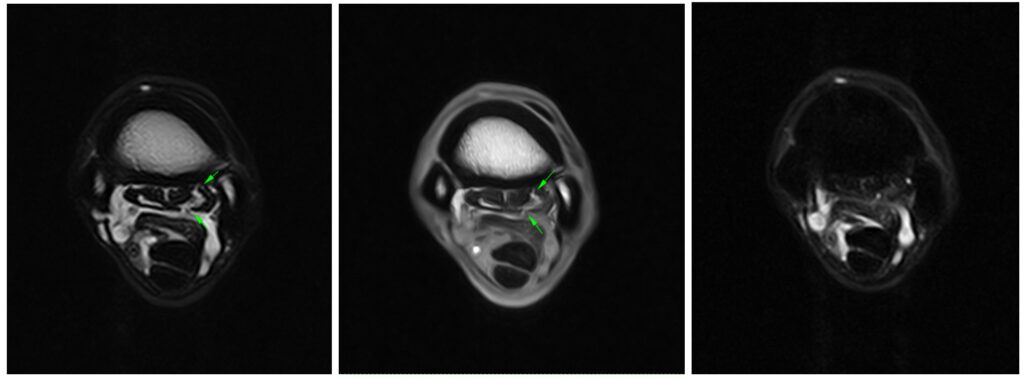
At the metacarpal region, there was an increased curvilinear signal intensity on all sequence types traversing the dorsal and palmar collagenous tissues of the lateral lobe of the proximal portion of the suspensory ligament. The dorsal margins of both lobes of the proximal portion of the suspensory ligament were slightly irregular. There was mild endosteal thickening of the palmar metacarpus medially with a small enthesophyte present.
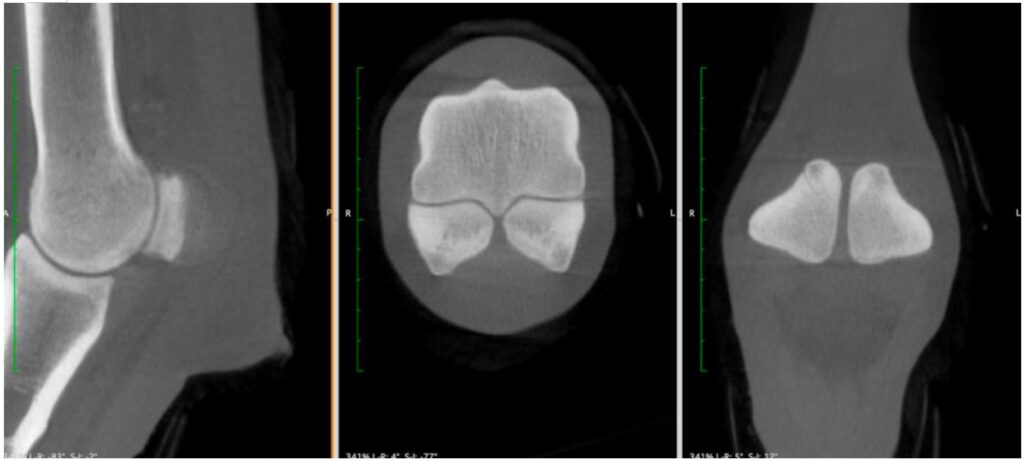
CT Findings
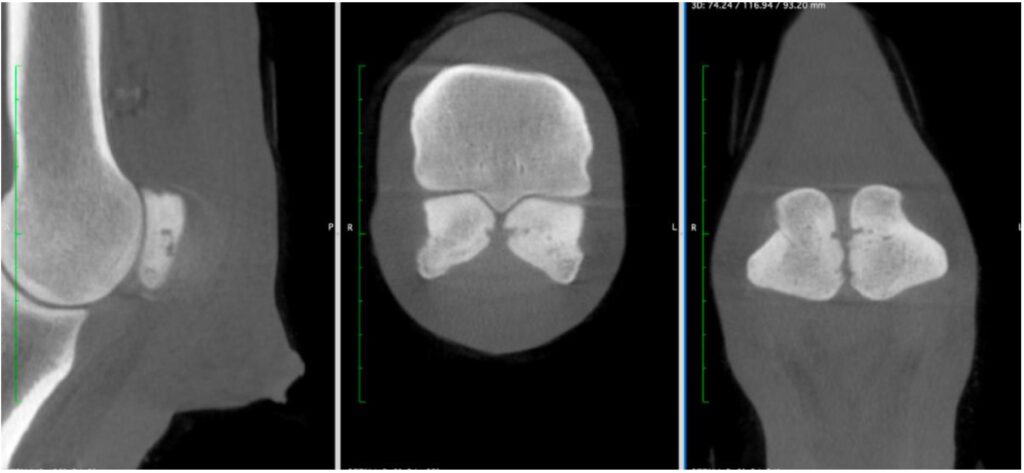
The horse underwent standing cone beam CT of the left front fetlock for further assessment of the changes within the proximal sesamoid bones. This revealed moderate sclerosis of the spongiosa of both proximal sesamoid bones (lateral greater than medial). There was irregular osteolysis at the axial margin of both the medial and lateral proximal sesamoid bones just over halfway up the bone. There was a further, smaller region of osteolysis within both proximal sesamoid bones distally. CT examination of the right fore fetlock revealed a normal appearance of the right proximal sesamoid bones.
Conclusion
The findings in the fetlock were consistent with desmopathy of the intersesamoidean ligament and mild axial osteitis of the proximal sesamoid bones. In the proximal metacarpal region, there were changes associated with very mild proximal suspensory ligament desmopathy.
Given the clinical nerve blocking pattern, the axial osteitis of the left fore proximal sesamoid bones and the intersesamoidean desmopathy were considered the most likely contributors to the current lameness.
With thanks to Dr. Sarah Taylor and Heather Pike, Dick Vet Equine Hospital, for sharing this case with us.
