


Spina Bifida of the Canine Sacrum
Spina bifida is a congenital (dorsal) cleft of the spinal column with or without protrusion of the meninges and sometimes the spinal cord. We look at a case in detail and discuss the use of veterinary CT and MRI in identifying neural and soft tissue defects.
The Patient
A 2-year-old female spayed German Shepherd dog was noted to have a ‘divot’ in the skin over her lumbosacral vertebral column since she was a puppy which had recently developed into a localized crusting reaction. She was evaluated by her primary veterinarian and had sedated radiographs done, which revealed spina bifida of her sacrum. Otherwise considered healthy, the dog underwent a vertebral column MRI using Hallmarq’s 2nd generation Small Animal 1.5T machine (see Figs 1 and 2).
The Imaging Results
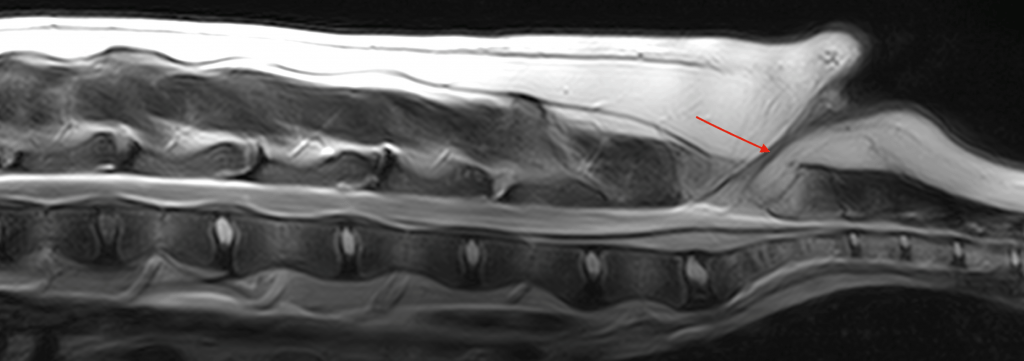
The intervertebral discs are hydrated being T2 weighted hyperintense and showing normal shape and position within their respective disc spaces. A linear hyperintensity contiguous with the dura extends dorsally at the level of the sacrum (arrow). The lesion is relatively well defined and appears to originate intradurally with extension to the dermis above it. There is no confirmed neural tissue within this CSF-filled extension, but this cannot be ruled out in these images. The soft tissue extension appears to be contained and does not exhibit a patency at its dorsal aspect. The skin at the site of the presumed attachment with the meningeal extension exhibits an indentation.
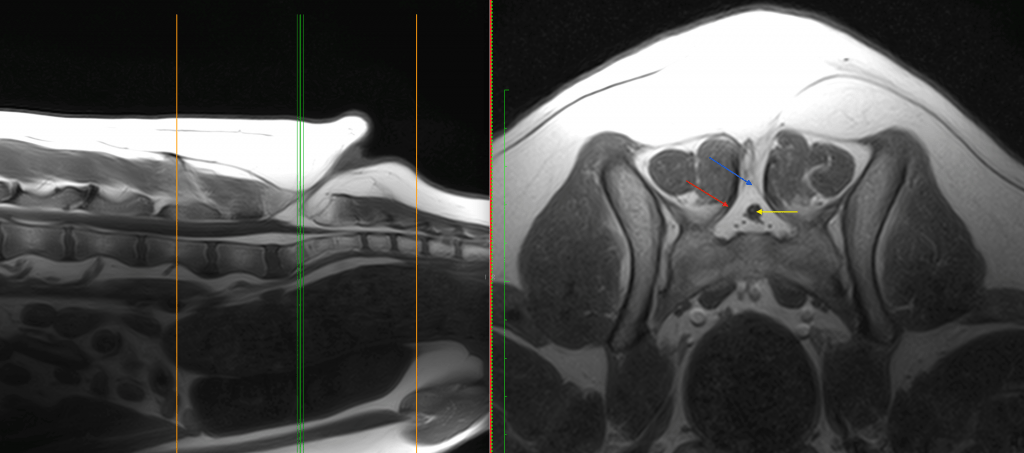
There is incomplete closure of the midportion of the dorsal lamina of S1 (red arrow; spina bifida). There is a funnel-like tract on the midline dorsal to the sacrum, extending in between the musculature toward the skin (blue arrow). The tract has a heterogeneous signal compared to muscle with a hypointense wall and hyperintense lumen. The conus medullaris can be seen in a normal position without deviation from the canal (yellow arrow). No contrast enhancement was noted on further imaging sequences.
Based on the images, surgical resection of the meningo(myelo)cele was performed and resection was determined to be complete based on the pathologist’s report. Descriptions of the surgical approach can be found in the references below. The dog recovered without any complication and, at her 2-week post-operative recheck, was assessed to be normal.
The Most Valuable MRI Sequence for This Case
The transverse T2W images allowed visualization of the tissue extending dorsally through the defect of the sacrum and the tissue contrast provided by the surrounding CSF allowed confirmation of the normal position of the conus within the canal.
Disease Overview
Spina bifida is a congenital (dorsal) cleft of the spinal column with or without protrusion of the meninges and sometimes the spinal cord. A meningocele is protrusion of meninges through a laminar defect in the spinal column forming a dural sac filled with cerebrospinal fluid, which was evident in the images in this case. A meningomyelocele is a protrusion of meninges and spinal cord or neural tissue through a defect in the spinal column.
The English bulldog and Manx cat are breeds predisposed with the lumbosacral area most commonly affected. Clinical signs reflect the involvement of the caudal lumbosacral intumescence or adjacent nerve roots. Clinical signs can also include a palpable dorsal vertebral defect caudally over the sacral area, a bunny hopping pelvic limb gait, plantigrade stance, paraparesis, pelvic limb ataxia, urinary or faecal incontinence, megacolon, atonic bladder, hyporeflexia of the pelvic limbs, anal sphincter, urinary bladder and sphincter, and alterations in nociception to perineal area and possibly to the pelvic limbs. The clinical suspicion requires confirmation with CT or MRI.
Conclusion
Although CT can assist with the 3-dimensional understanding of the bony defect, the neural and soft tissue defect requires MR imaging to be identified, especially if resection surgery is to be considered. The use of contrast is essential to investigate the possibility of associated infections if the defect is open to the environment. As a result, surgical treatment is suggested in dogs with clinical signs and results in outcomes ranging from an unchanged neurological condition to (rarely) return to normal function.
With thanks to the Diagnostic Imaging Team at Veterinary Emergency + Referral Center, Honolulu, Hawaii for providing this case study.
References
- Kopke MA, Jack MW, Baltzer WI, Wightman PF, Gal A. Dermoid sinus type VI associated with spina bifida and tethered cord syndrome in a French Bulldog. J Vet Diagn Invest. 2019 Mar;31(2):294-297. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6838840/
- Martín Muñiz L, Del Magno S, Gandini G, Pisoni L, Menchetti M, Foglia A, Ródenas S. Surgical outcomes of six bulldogs with spinal lumbosacral meningomyelocele or meningocele. Vet Surg. 2020 Jan;49(1):200-206
- Song RB, Glass EN, Kent M. Spina Bifida, Meningomyelocele, and Meningocele. Vet Clin North Am Small Anim Pract. 2016 Mar;46(2):327-45
