


Spinal subarachnoid diverticula (SAD) are fluid dilations in the subarachnoid space that can cause compression of the spinal cord and an associated myelopathy. In this study, from Tucson Veterinary Specialists, we take a look at how 1.5T MRI proved invaluable in aiding diagnosis for this case.
The Patient
A 6-year-old female French bulldog presented with a 2-3 month history of progressive asymmetric pelvic limb weakness and a recent onset of faecal incontinence.
Radiographs of her thoracolumbar vertebral column showed typical malformations of French bulldogs with mid-thoracic kyphosis and shortened vertebral bodies affecting T7, T8, and T9, compatible with hemivertebrae (Fig.1).
In addition, there was narrowing of the T13-L1 intervertebral disc space. As a result, intervertebral disc disease and the effects of the vertebral malformations on the cord were considered at this time. Accordingly, medical management was advised as the dog was still ambulatory, but continued neurologic progression was observed.
Otherwise considered healthy, the dog underwent a thoracolumbar vertebral column MRI using the Hallmarq 1.5T MRI machine (see Fig. 2).
The Imaging Results

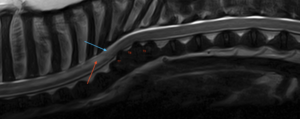
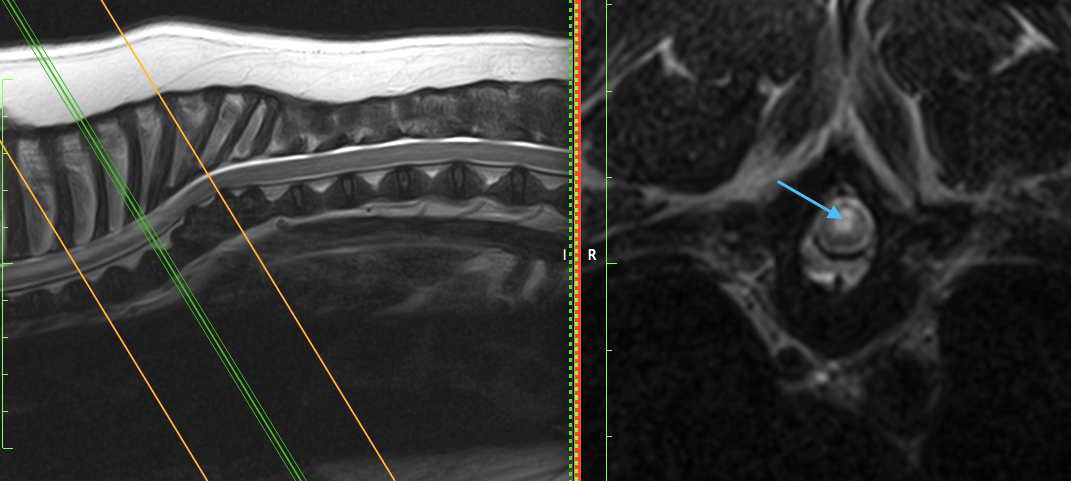
Fig 2c: (right) A T2W transverse image of the vertebral column at the level of T6-T7. There is a relatively well-defined intradural expansion dorsal to the cord, more prominent on the left, with mild underlying cord compression (blue arrow).
There is an ill-defined and irregular ventral extradural lesion over the disc space, which is T2W hypointense and associated with obliteration of the ventral subarachnoid space (red arrow).
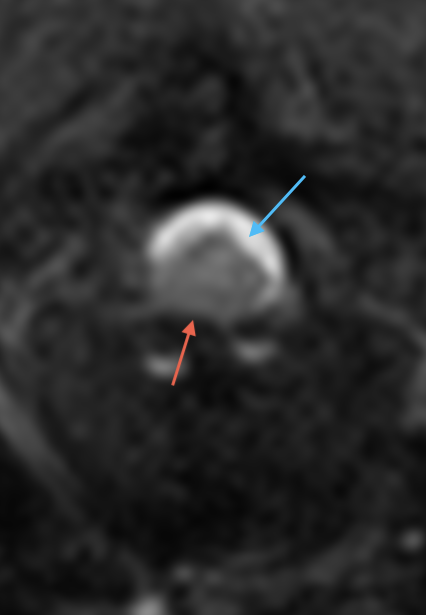
Based on the images, a dorsal subarachnoid diverticulum was suspected at T6-T7 with an intramedullary myelopathy cranial to the lesion, suggestive of a pre-syrinx.
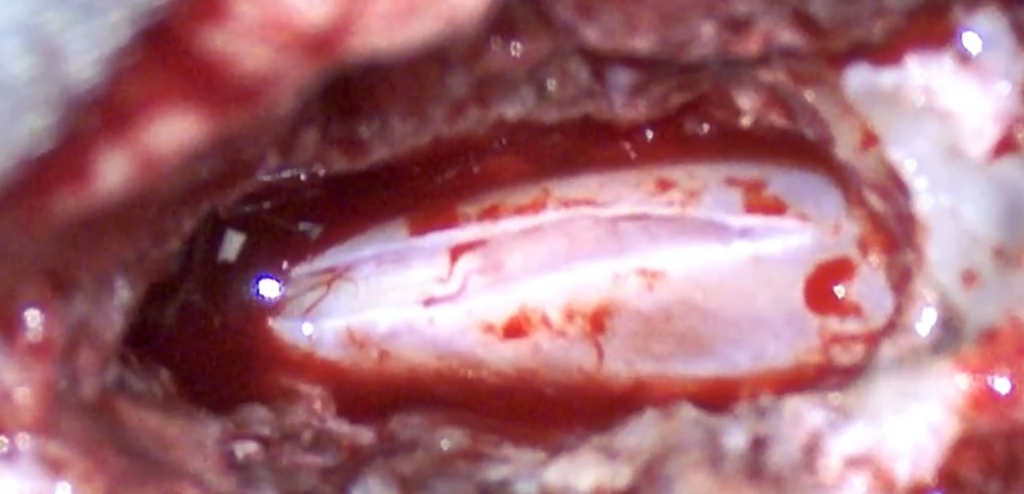
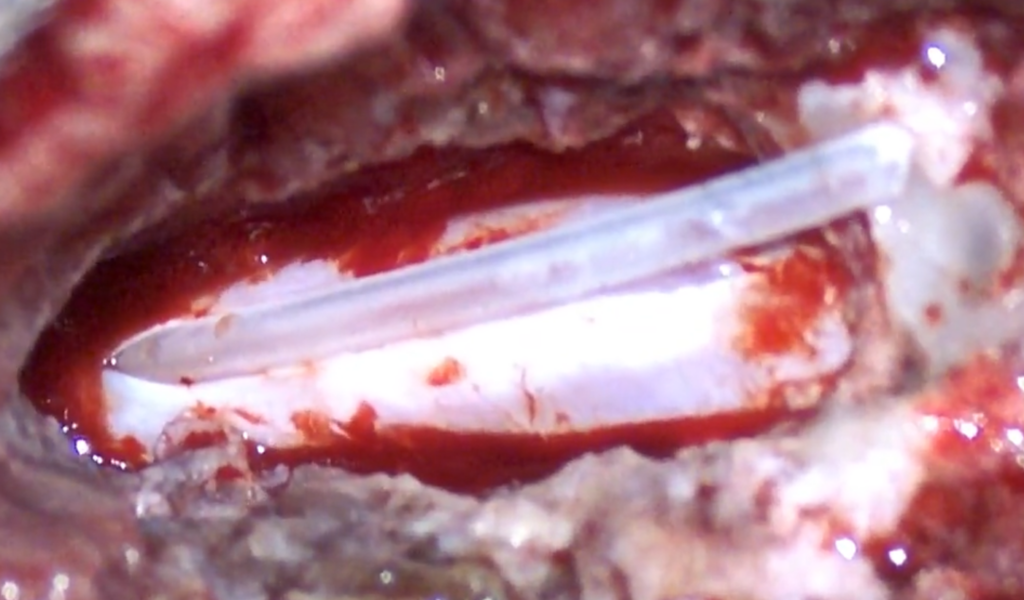
A surgical implantation of a subarachnoid shunt was performed at the level of the diverticulum (Fig 3.). Descriptions of the surgical approach can be found in the references below. The dog recovered without any complications, and at her 2-week post-operative recheck, was assessed to be stable.
Spinal subarachnoid diverticula: a disease overview
Spinal subarachnoid diverticula (SAD) are fluid dilations in the subarachnoid space that can cause compression of the spinal cord and an associated myelopathy. In humans, these diverticula make up 1% to 3% of all mass-like lesions of the spinal canal and, although considered rare in dogs, the overall incidence has not been reported. The aetiology remains unknown, with broad categories of congenital and acquired subarachnoid diverticula being described. Associated leptomeningeal adhesions and arachnoid webs have been reported in conjunction with SAD in dogs and humans. Arachnoid webs are rare intradural pathologies that share many imaging and intraoperative similarities with the canine SAD. Thoracolumbar and cervical spinal cord segments are most commonly affected with clinical signs consistent with a progressive myelopathy in these regions.
Certain breeds, most notably pugs, rottweilers, and French bulldogs, are over-represented in the literature. Pugs make up 28% (92/324), rottweilers 19% (62/324), and French bulldogs 13% (43/324) of the reported cases that identified the breed of dog. This suggests a genetic or hereditary cause for subarachnoid diverticula formation.
Progressive proprioceptive ataxia and paresis from compressive thoracolumbar myelopathy, as well as urinary and fecal incontinence, are common, particularly with thoracolumbar lesions, and pain is less common than in many other spinal disorders.
1.5T MRI for Thoracolumbar Subarachnoid Diverticulum
MRI findings typically show dorsal or dorsolateral subarachnoid space widening, CSF-like signal that is T2 hyperintense and T1 hypo-/isointense, and spinal cord compression. In addition, MRI also helps detect associated intramedullary T2 hyperintensity, syringomyelia, vertebral malformations, disc protrusion, or other concurrent lesions that may affect prognosis and surgical planning.
Thoracolumbar SAD often coexists with other structural problems rather than appearing as an isolated lesion. CT or CT-myelography can add value when vertebral malformation, caudal articular process dysplasia, instability, or disc disease is suspected
Several treatment options have been documented with variable short and long-term success. See the table below:
| Approach | Reported Findings | Key Caveat |
| Durotomy/durectomy with adhesion dissection | Commonly improves neurologic function short term | Recurrence can still occur months to years later |
| Shunt-based surgery | 85.7% improved long term with lower recurrence than durotomy alone | Immediate postoperative worsening is more common after shunts |
| Stabilization when dynamic lesion exists | Some dogs improved for 49-126 months after stabilization-based surgery | Evidence is limited to small series and selected cases |
| Medical management alone | Improvement occurs in a minority of dogs overall | Long-term outcomes are generally worse than surgery |
Immediate postoperative deterioration is recognized, especially in Pugs and after shunt placement, but many dogs recover walking ability within weeks. However, long-term prognosis is the main uncertainty. General canine series favor surgery, but Pugs have distinctly worse long-term outcomes, with frequent recurrence or later deterioration and possible contributions from syringomyelia, fibrosis, or concurrent vertebral disease.
With thanks to Cody Alcott, DVM, and the team at Tucson Veterinary Specialists for sharing this study.
References
- Aikawa T, Shimatsu T, Miyazaki Y. Hemilaminectomy, Diverticular Marsupialization, and Vertebral Stabilization for Thoracolumbar Spinal Arachnoid Diverticula in Five Dogs. Journal of the American Animal Hospital Association. 2019 Feb;55(2):110–116
- Gomes SA, Targett M, Mignan T, et al. Post-surgical outcome and recurrence rates in thoracolumbar arachnoid diverticula undergoing durotomy alone or alongside a modified technique of subdural shunt-placement in dogs. Veterinary Surgery. 2025;54(5):972-982
- Neringa Alisauskaite, Sigitas Cizinauskas, Janis Jeserevics, Mindaugas Rakauskas, Giunio Bruto Cherubini, Marjukka Anttila, Frank Steffen, Short- and long-term outcome and magnetic resonance imaging findings after surgical treatment of thoracolumbar spinal arachnoid diverticula in 25 Pugs, Journal of Veterinary Internal Medicine, Volume 33, Issue 3, May-June 2019, Pages 1376–1383
- Jones, B., Behr, S., Shaw, T., Cappello, R., Jeffery, N., Liebel, F.X. and Harcourt-Brown, T. (2022), Surgical techniques used in the management of intra-arachnoid diverticula in dogs across four referral centres and their immediate outcome. J Small Anim Pract, 63: 520-525.
- D.A. Mauler, S. De Decker, L. De Risio, H.A. Volk, R. Dennis, I. Gielen, E. Van der Vekens, K. Goethals, L. Van Ham, Spinal Arachnoid Diverticula: Outcome in 96 Medically or Surgically Treated Dogs, Journal of Veterinary Internal Medicine, Volume 31, Issue 3, May-June 2017, Pages 849–85
