


Although individual studies vary, brain tumours – or gliomas – represent between 36% to 70% of primary brain tumours in dogs. Over 50% of all gliomas in dogs occur in certain brachycephalic breeds. These include Boston Terriers, Bulldogs, and Boxer dogs. With gliomas difficult to identify using CT, MRI is the preferred imaging modality for evaluation of intracranial lesions.
The patient
A 5-year-old male neutered French Bulldog presented for an onset of cluster seizure activity. The neurological examination was considered normal at the time of presentation. Otherwise considered healthy, the dog underwent a brain MRI using the Hallmarq 1.5T machine (Fig. 1).
Based on these images supporting a suspected diagnosis of an intracranial glioma, a craniectomy for mass resection was performed, which confirmed an astrocytoma. The surgery was followed by stereotactic radiotherapy 3 weeks later. Repeat imaging was undertaken 2 weeks after the surgery (Figures 2B & 3B), 6 months after the radiotherapy (Figures 2C & 3C), and 1 year after the radiotherapy (Figures 2D & 3D).
The imaging results
Figure 1. Transverse MR images at the level of the occipital lobes at the time of the dog’s initial presentation. (A) T2W; (B) FLAIR; (C) T1W; and (D) T2* sequences. A large, ill-defined and multi-compartmental intraparenchymal lesion is seen at the level of the occipital lobe on the left side. The lateral component of the lesion is heterogeneously T2W, T2*, and FLAIR hyperintense to grey matter with irregular intralesional hypointensities on all sequences.
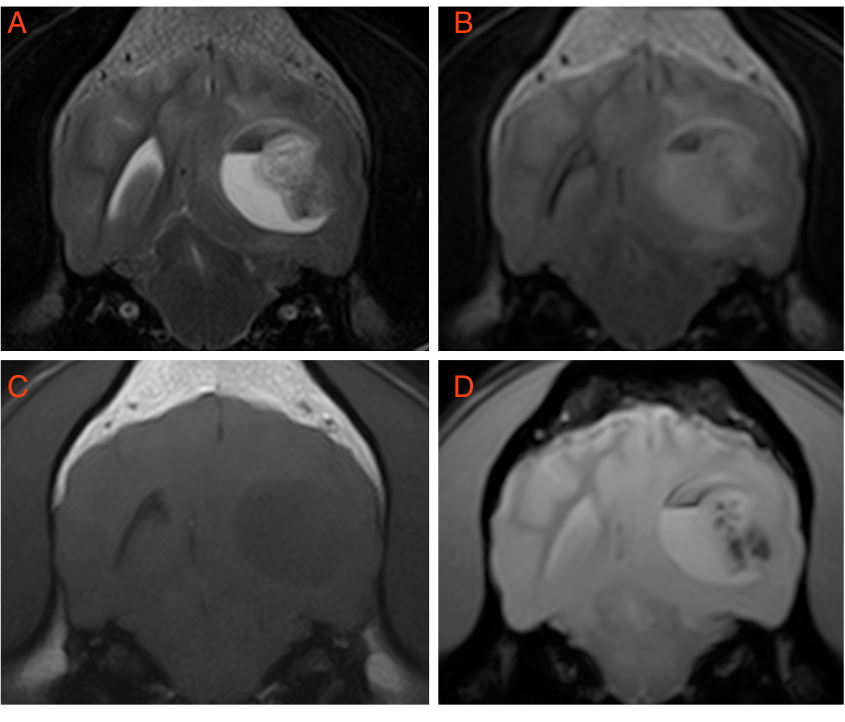
The medial portion of the mass is more well-defined with a distinct fluid line near its dorsal aspect. The ventral portion is homogeneously hyperintense on all sequences apart from being mildly hypointense on T1W. The dorsal aspect is hypointense on T2W and FLAIR, mildly hypointense on T1W with mixed to hyperintense signal on T2*. This medial portion represents a highly proteinaceous cystic component with suspected dorsal haemorrhage. The main differentials for this mass lesion would include high-grade glioma and, less likely, an inflammatory granuloma.
Figure 2. Transverse T2W images at the level of the occipital lobes acquired at the time of presentation (A), 2 weeks after surgery (B), 6 months after surgery and radiation therapy (C), and 1 year after surgery and radiation therapy (D). The bone defect in the overlying calvaria secondary to surgery can be seen (arrow). The soft tissue lateral mass is smaller post-surgery, but is not detectable after radiation. A cystic lesion remains after radiation (C & D).
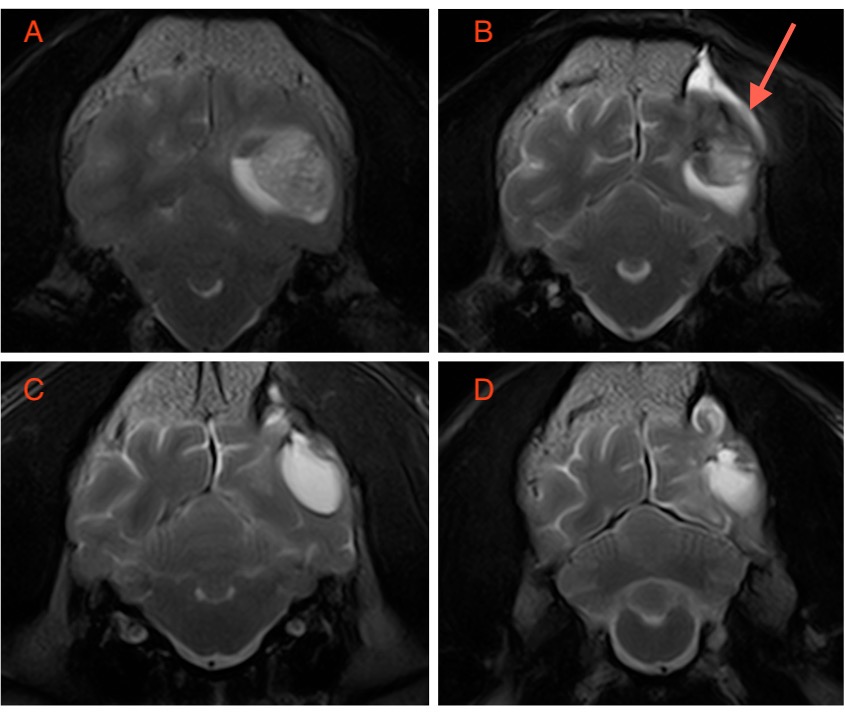
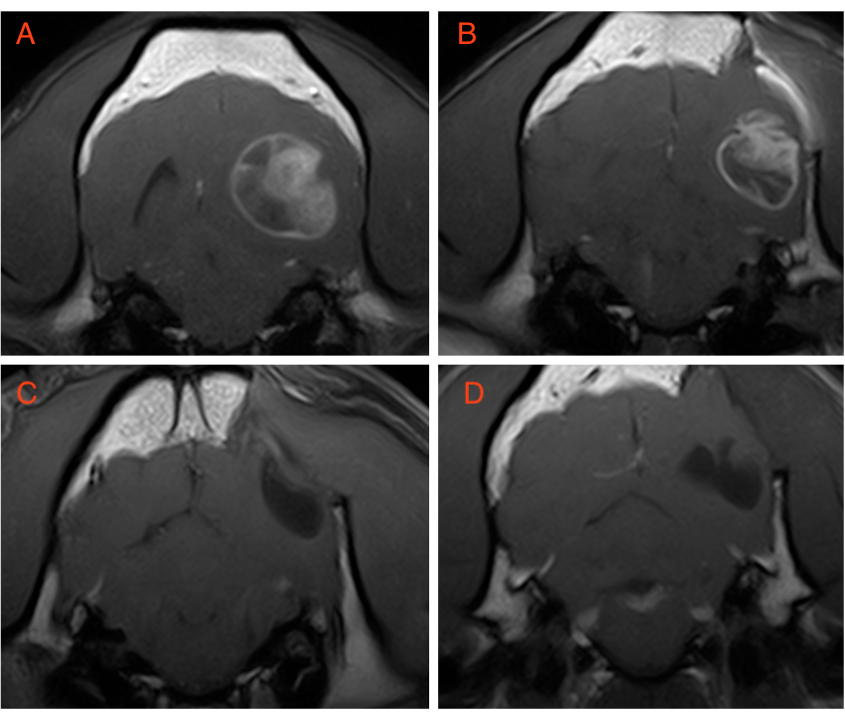
Figure 3. Transverse T1W post-contrast images at the level of the occipital lobes acquired at the time of presentation (A), 2 weeks after surgery (B), 6 months after surgery and radiation therapy (C), and 1 year after surgery and radiation therapy (D). The soft tissue component contrast enhances strongly but heterogeneously pre- and post-surgery, but is not seen after radiation therapy. The rest of the lesion peripherally enhances, and this also is not seen after radiation.
The most valuable MRI sequence for this case
The T1W post-contrast sequence demonstrates the ‘true’ extent of the disease, with T2W and FLAIR helping to identify peri-lesional oedema. The lack of contrast enhancement around the remaining cystic lesion in this case, following radiation, suggests a markedly reduced tumour burden, which is not possible to assess using some of the other sequences.
Disease overview
Although individual studies vary, gliomas represent 36% to 70% of primary brain tumours in dogs. Epidemiologic data on glioma in dogs indicate a median age at diagnosis of 8 years, a male predilection (incidence ratio of 1.53 for males/females), and predominant lesion location within the fronto-olfactory, temporal, and parietal lobes of the brain.1,2 Over 50% of all gliomas in dogs occur in certain brachycephalic breeds. These include Boston Terriers, Bulldogs, and Boxer dogs.
Gliomas arise from the supporting cells of the brain parenchyma (e.g., extra-parenchymal location). These include astrocytes and oligodendrocytes, forming astrocytomas and oligodendrogliomas, respectively. Gliomas are further divided into low- or high-grade. Among contrast-enhancing gliomas, the patterns and degree of enhancement seen can be highly variable. A “ring enhancing” pattern, as seen in this case, in which a circular ring of contrast enhancement surrounds non-enhancing abnormal tissue, is often associated with gliomas.
However, ring enhancement is a non-specific finding that has been associated with several neoplastic, vascular, and inflammatory brain diseases. High-grade gliomas are more likely to demonstrate contrast enhancement. Gliomas can be difficult to identify using CT, thus MRI is the preferred imaging modality for the evaluation of intracranial lesions. However, gliomas can appear similar to other intracranial diseases such as inflammatory granulomas. The latter is more likely to exhibit dural contact, T2-hypointensity, concomitant meningeal enhancement, and minor changes in the contralateral brain.
A study of 91 dogs with CNS glioma found that definitive treatments were associated with significantly longer survival (median survival time 84 days) than palliative treatment (26 days).1 Another previous study reported a median survival time of 66 days after surgical resection alone in 14 gliomas.3
Survival time was recently investigated in 38 dogs with suspected symptomatic primary solitary intracranial glioma, treated with a complete uniform fractionated megavoltage radiation protocol of 15x3Gy over 5 weeks.4 The disease-specific median survival time was 698 days. Survival at 1 and 2 years was 74.2% and 49.0%.
With thanks to Dr. Baye Williamson DACIVM (Neurology) and team at Veterinary Emergency + Referral Center (VERC), Hawaii for this study.
References
- José-López R, Gutierrez-Quintana R, de la Fuente C, et al. Clinical features, diagnosis, and survival analysis of dogs with glioma. J Vet Intern Med. 2021; 35(4): 1902–1917
- Song RB, Vite CH, Bradle CW, et al. Postmortem evaluation of 435 cases of intracranial neoplasia in dogs and relationship of neoplasm with breed, age and body weight. J Vet Intern Med. 2013; 27: 1143-1152.
- Suñol A, Mascort J, Font C, et al. Long-term follow-up of surgical resection alone for primary intracranial rostrotentorial tumors in dogs: 29 cases (2002-2013). Open Vet J. 2017; 7: 375-383.
- Debreuque M, De Fornel P, David I, Delisle F, Ducerveau MN, Devauchelle P, Thibaud JL. Definitive-intent uniform megavoltage fractioned radiotherapy protocol for presumed canine intracranial gliomas: retrospective analysis of survival and prognostic factors in 38 cases (2013-2019). BMC Vet Res. 2020 Oct 31;16(1):412.


