

Solar abscess from right hind foot
History
A 9-year-old broodmare was MRI’d due to a persistently draining solar abscess from her right hind foot which, after 3 weeks of routine abscess management, was not improving.
Case 1 – MRI Findings
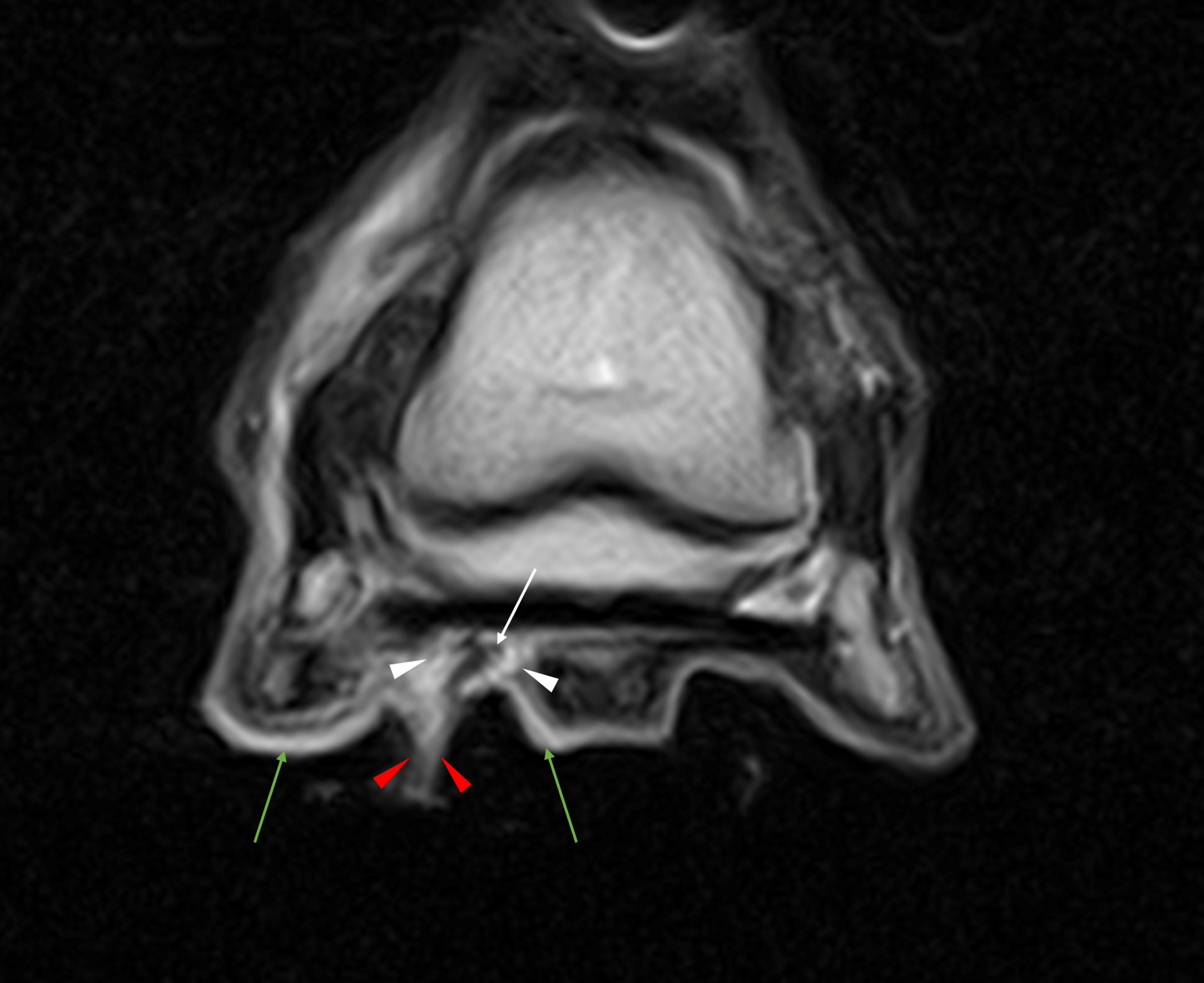
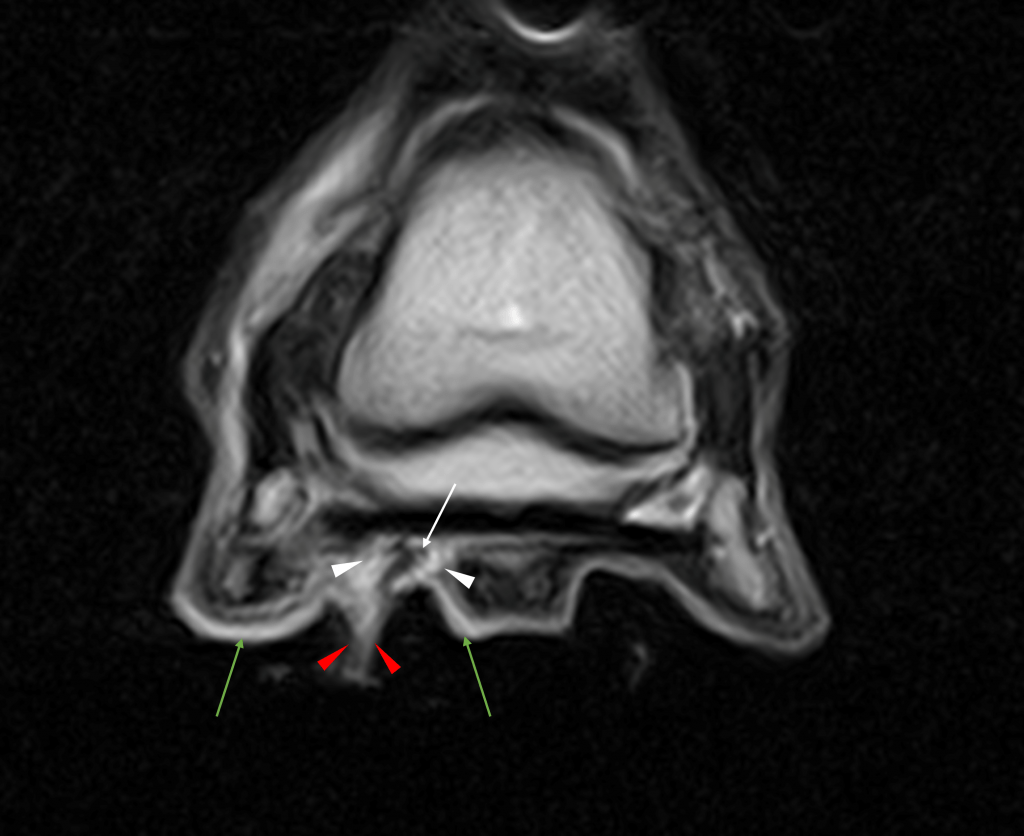
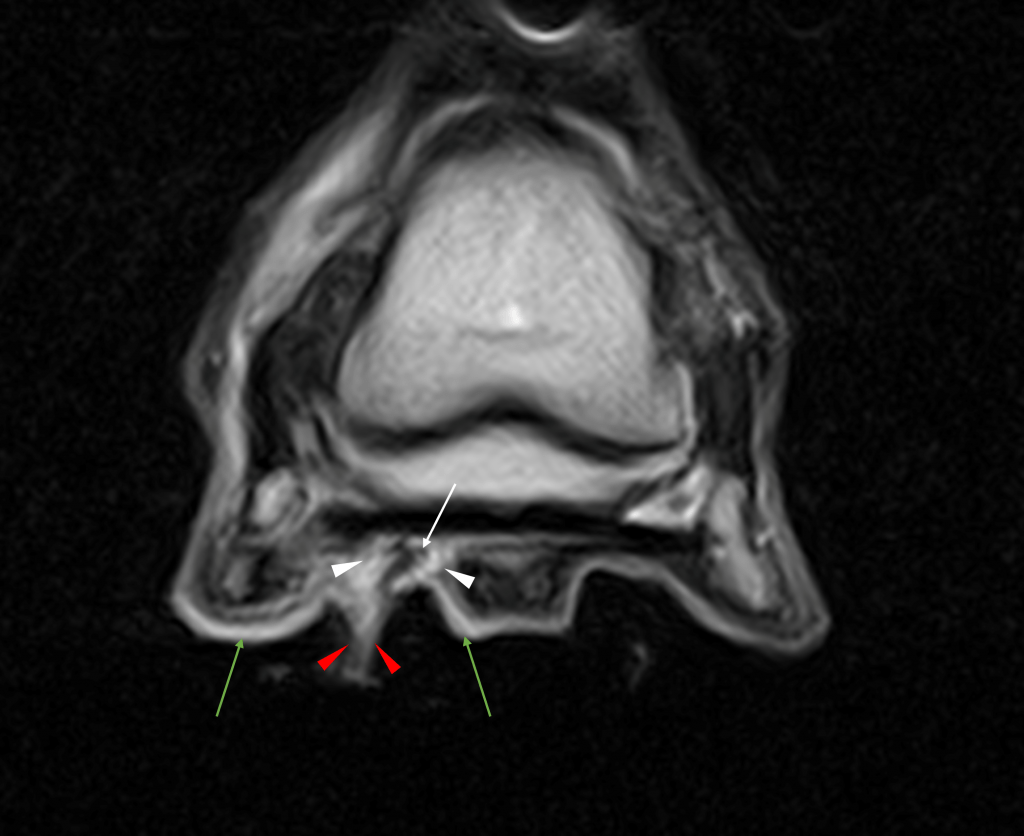
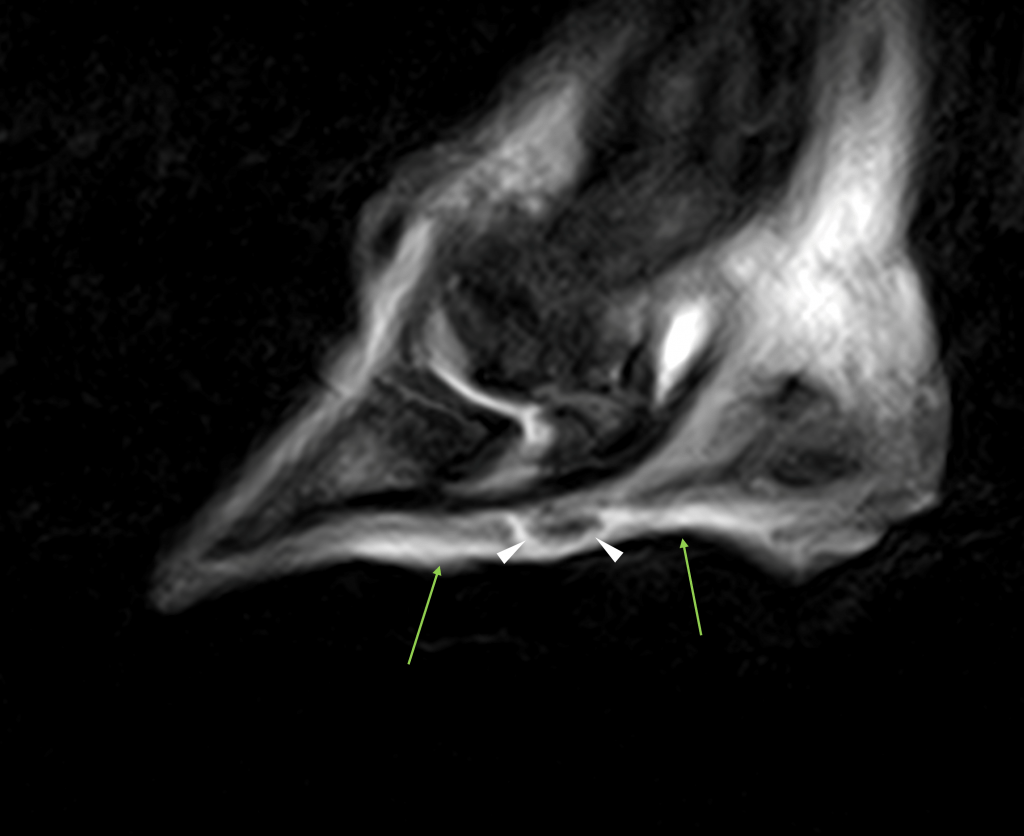
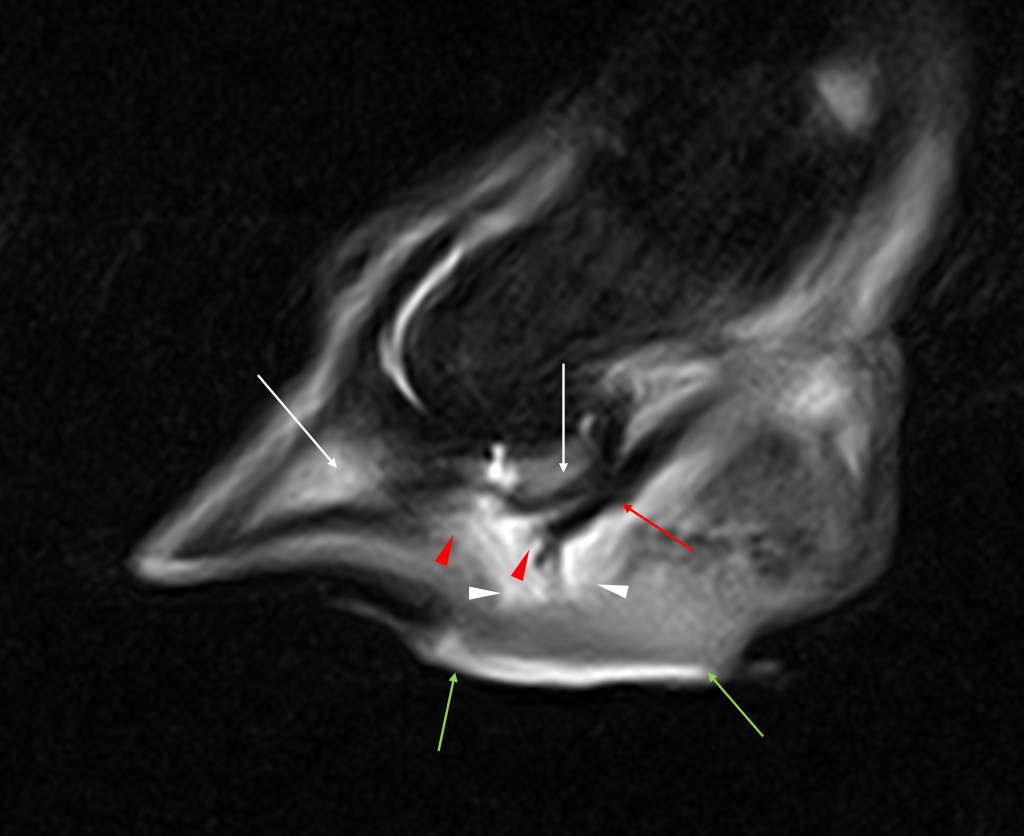
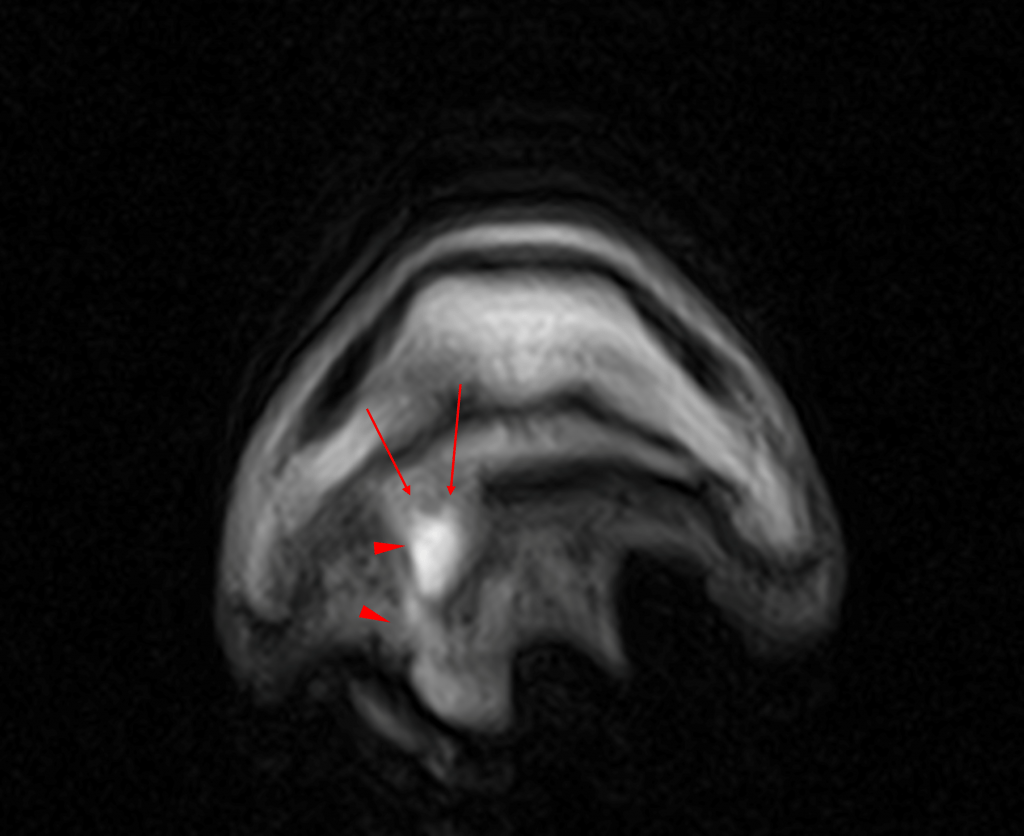
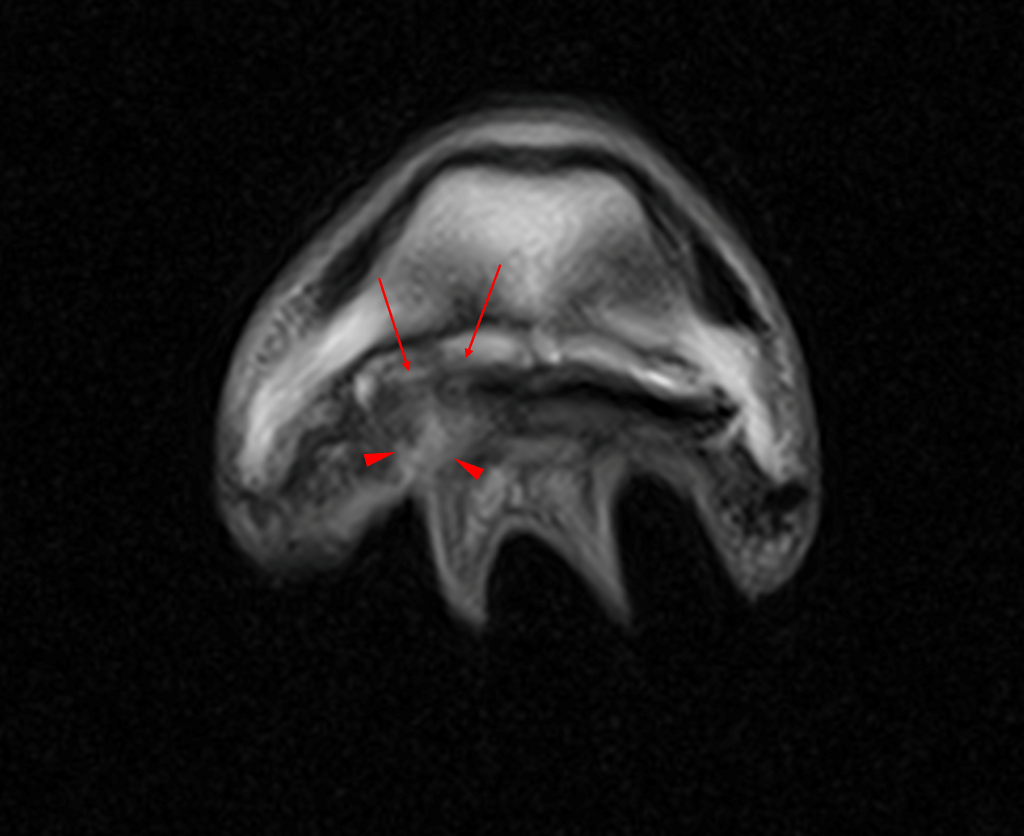
As expected, STIR and T2 FSE images revealed a hypointense pocket in the solar dermis (white arrow) surrounded by a halo of signal hyperintensity (white arrowheads) indicating the region of subsolar hemorrhage and infection. The location of this pocket and halo, the focal point of infection, was shown to be within the soft tissue at the plantar border of the most distal aspect of the deep digital flexor tendon. The signal intensity within the tendon, fortunately, appeared normal.
On the same images, draining material was shown to be exiting close to the lateral sulcus of the frog (red arrowheads). The solar dermis was diffusely hyperintense and thick (green arrows), again consistent with diffuse inflammation and subsolar infection.
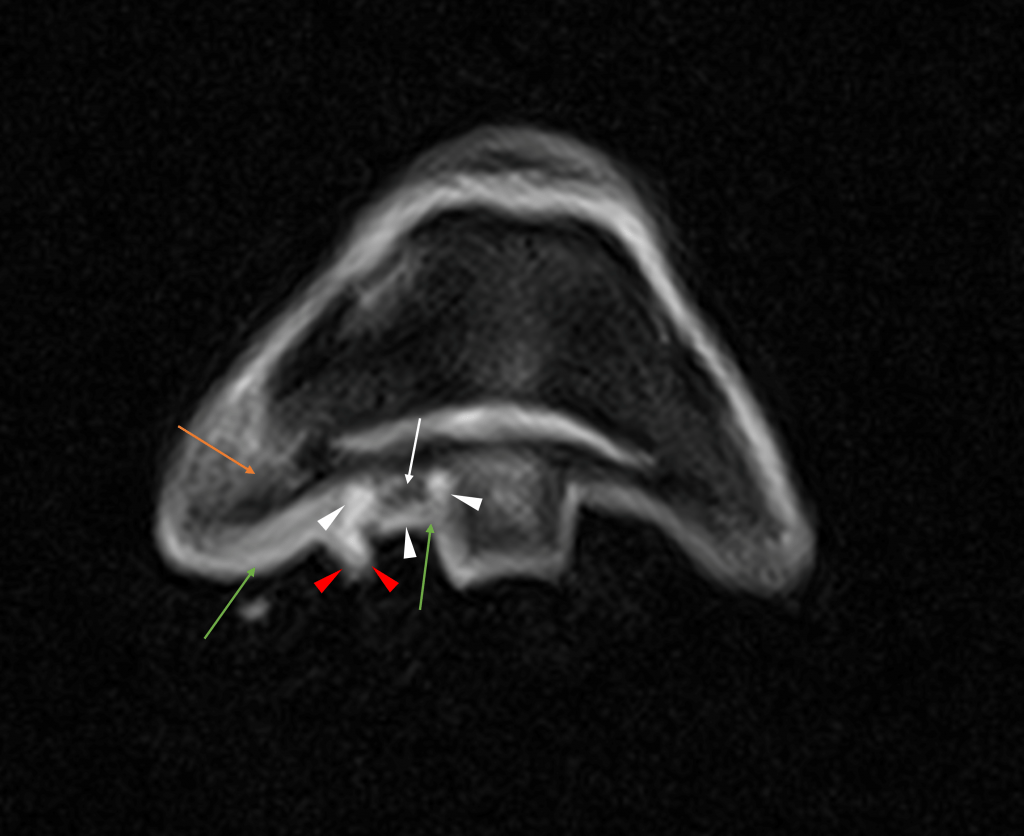
The above left-handed STIR image shows a diffuse fluid signal in the lateral palmar process of the distal phalanx, extending to the body of the phalanx (orange arrow). Which may indicate inflammation or infection within the phalanx.
The deep digital flexor tendon was of normal appearance on all sequences.
The navicular bursa was moderately distended but otherwise of normal appearance.
Conclusions
- Subsolar infection and draining tract in the lateral sulcus, the focus of this infection being extremely close to the DDFT.
- Inflammation or possibly septic osteitis of the pedal bone.
- Diffuse inflammation in the solar dermis is consistent with subsolar injection.
- Synovial involvement was considered unlikely.
- Advice was given to carry out synoviocentesis.
Case 2 – MRI Findings
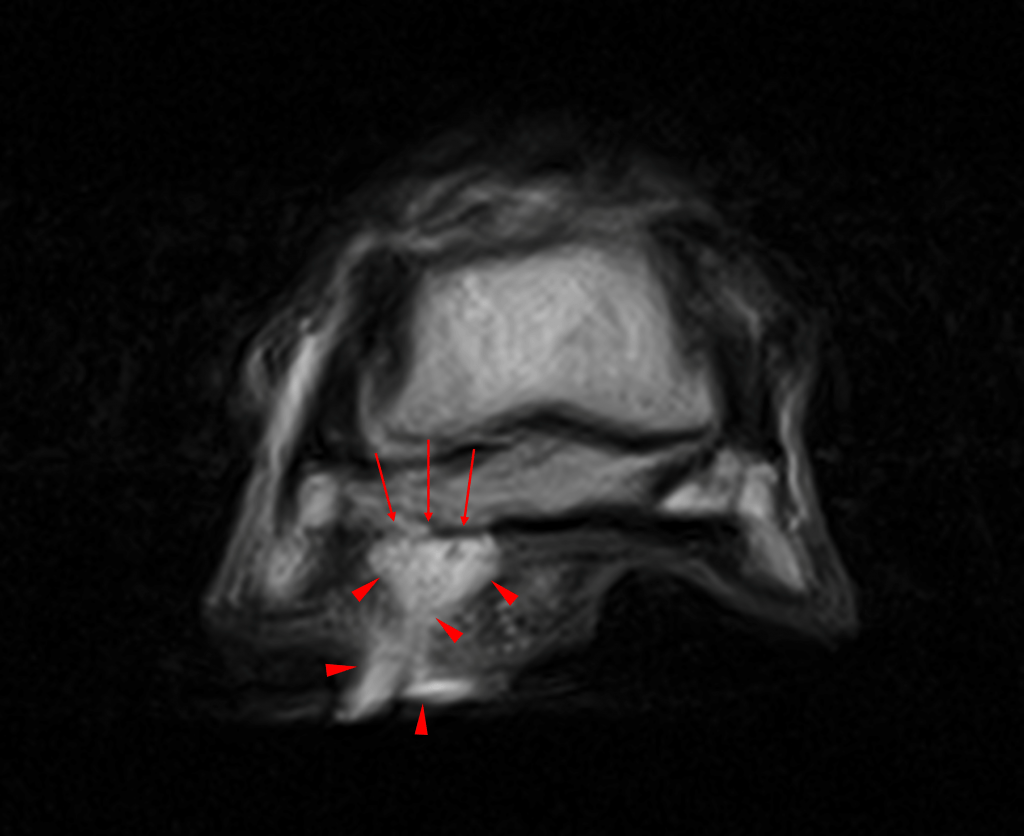
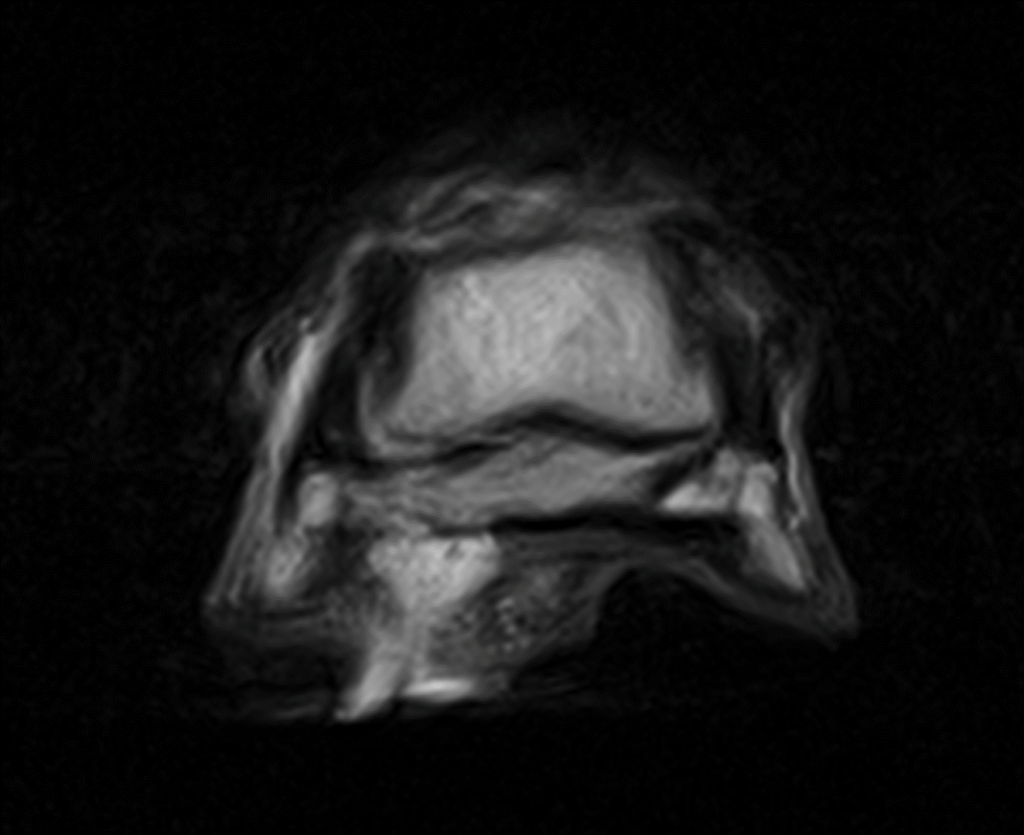
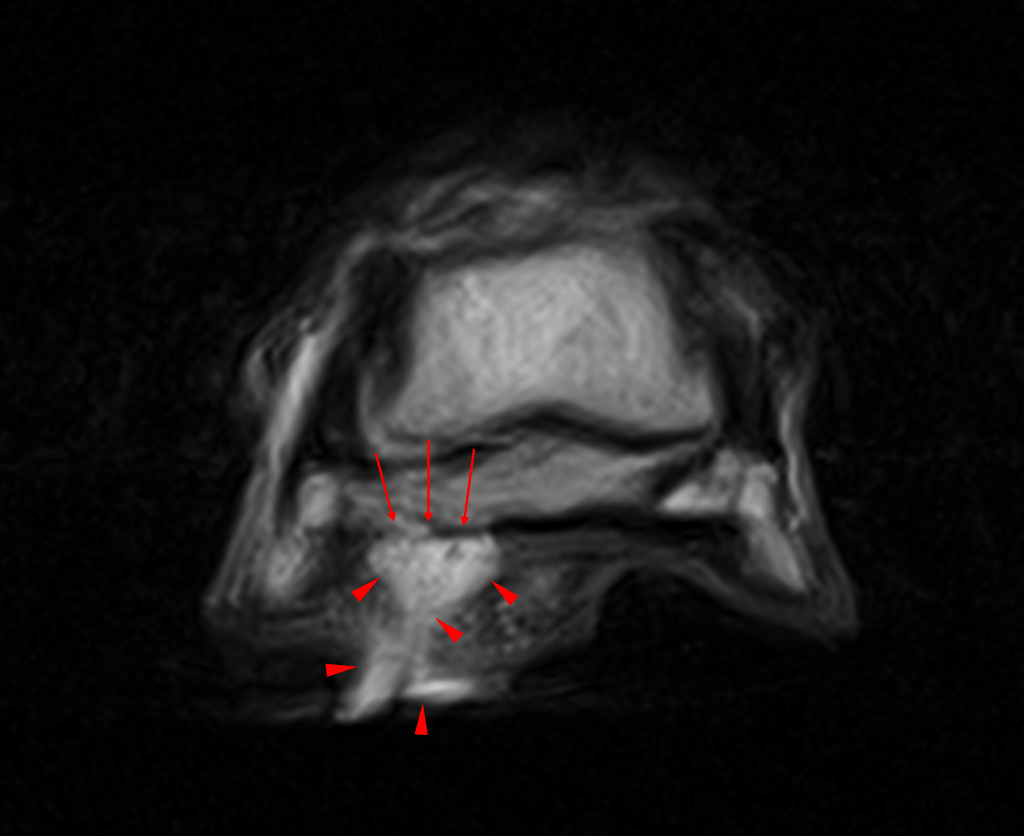
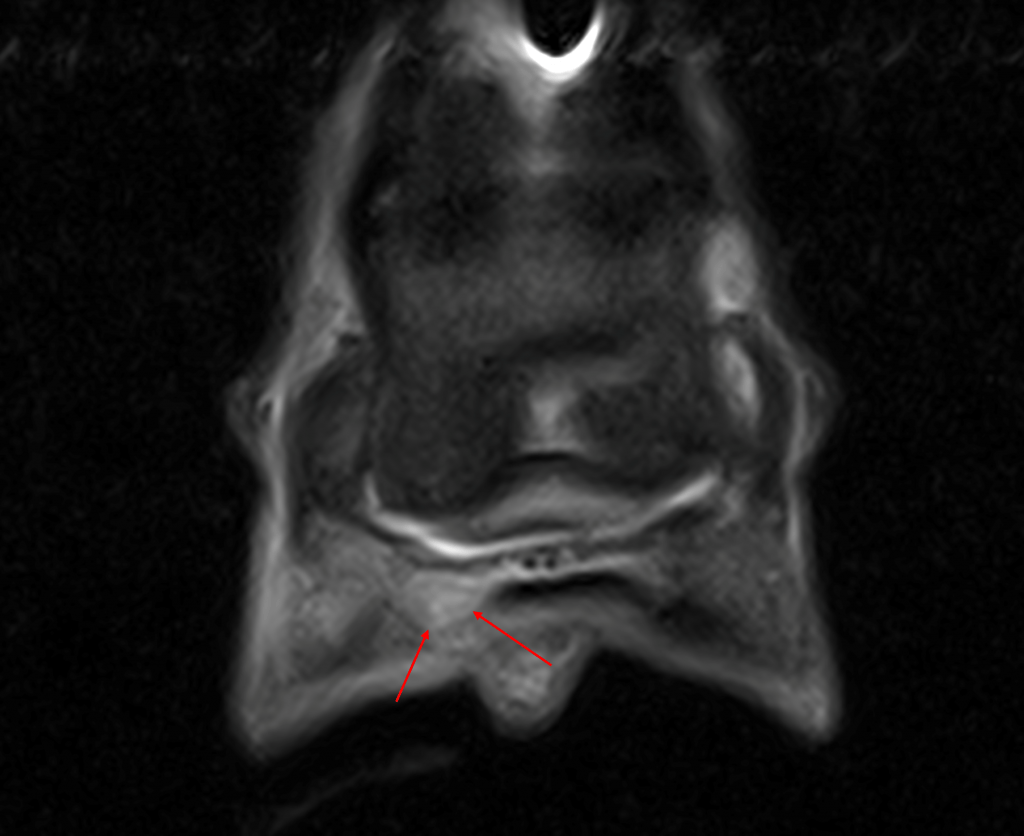
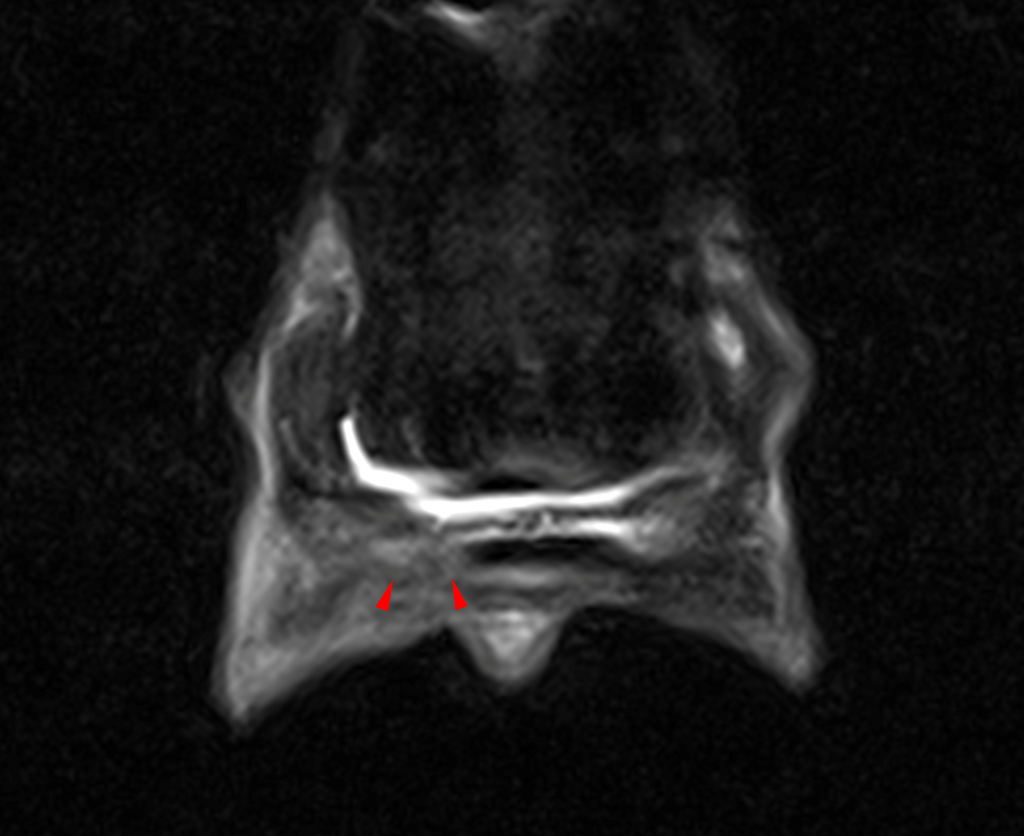
Repeat MRI a fortnight later (right image) revealed the draining tract to be larger (red arrowheads) compared to previous (left image) on the T2FSE frontal images. Additionally, a distinct loss of integrity of the lateral part of deep digital flexor tendon towards its insertion was visible (red arrows). This loss of integrity to the tendon was present from the level of the navicular bone to the insertion on the distal phalanx.
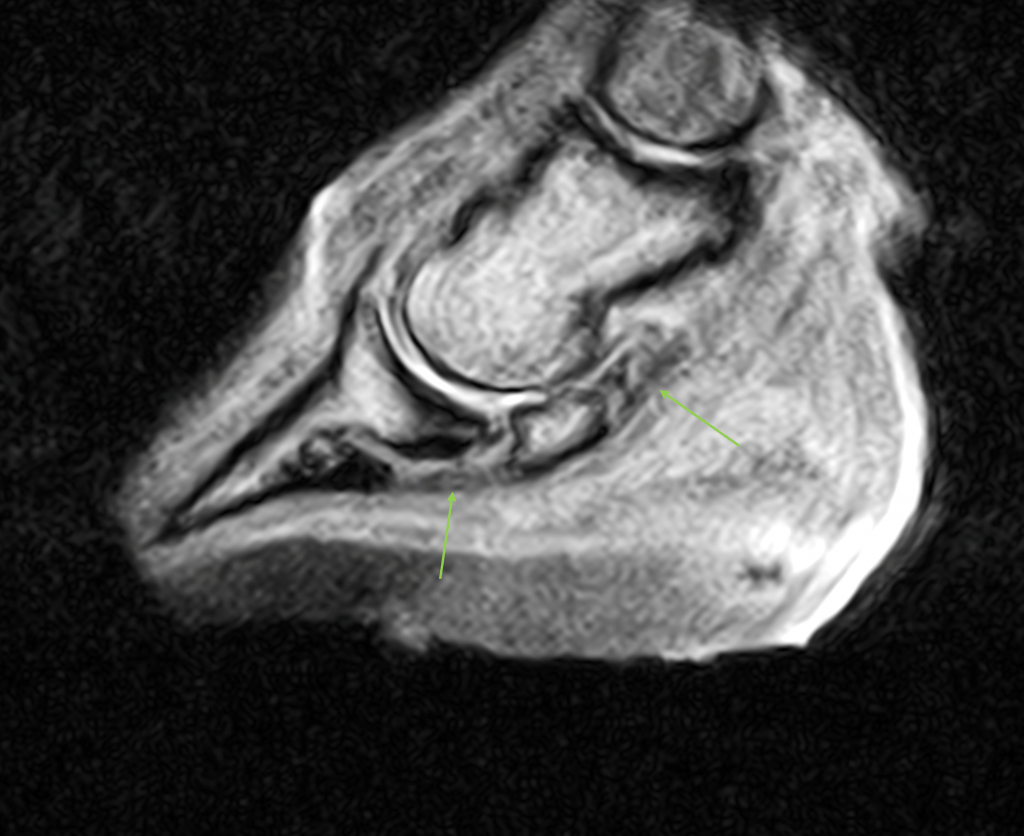
The T1 sagittal images with the previous scan to the left and the most recent to the right demonstrate the loss of integrity of the tendon distal to the navicular bone (green arrows). Fluid signal within the solar tissues and disruption of the architecture of the solar dermis and margin is demonstrated by the red arrowheads.
The previously localised interosseous signal on the below sagittal STIR images (previous scan to the left, recent scan to the right) was now diffuse within the distal phalanx and the navicular bone (white arrows), and the navicular bursa more distended. The green arrows highlighting the hyperintensity in the solar tissues show the increase in the inflammatory response within the solar dermis. The hypointense focus previously seen very close to the DDFT (white arrowheads) had been replaced by amorphous fluid signal intensity consistent with infection and possibly granulation tissue.
Conclusions
- Septic deep digital flexor tendinopathy with partial rupture of the fibres in the lateral aspect of the terminal portion of the DDFT.
- Navicular bursitis. Synoviocentesis is always required to rule out synovial sepsis.
- Draining tract and granulation tissue formation.
- Marked inflammation of the distal phalanx and navicular bone, most likely due to the marked inflammatory process within the foot. Septic osteitis/osteomyelitis could not be excluded.
Case 3 – MRI Findings
The hyperintense (soft tissue/fluid signal intensity) tract was now less extensive as shown by the red arrowheads in the T2 FSE frontal images below with the previous images to the left and recent to the right.
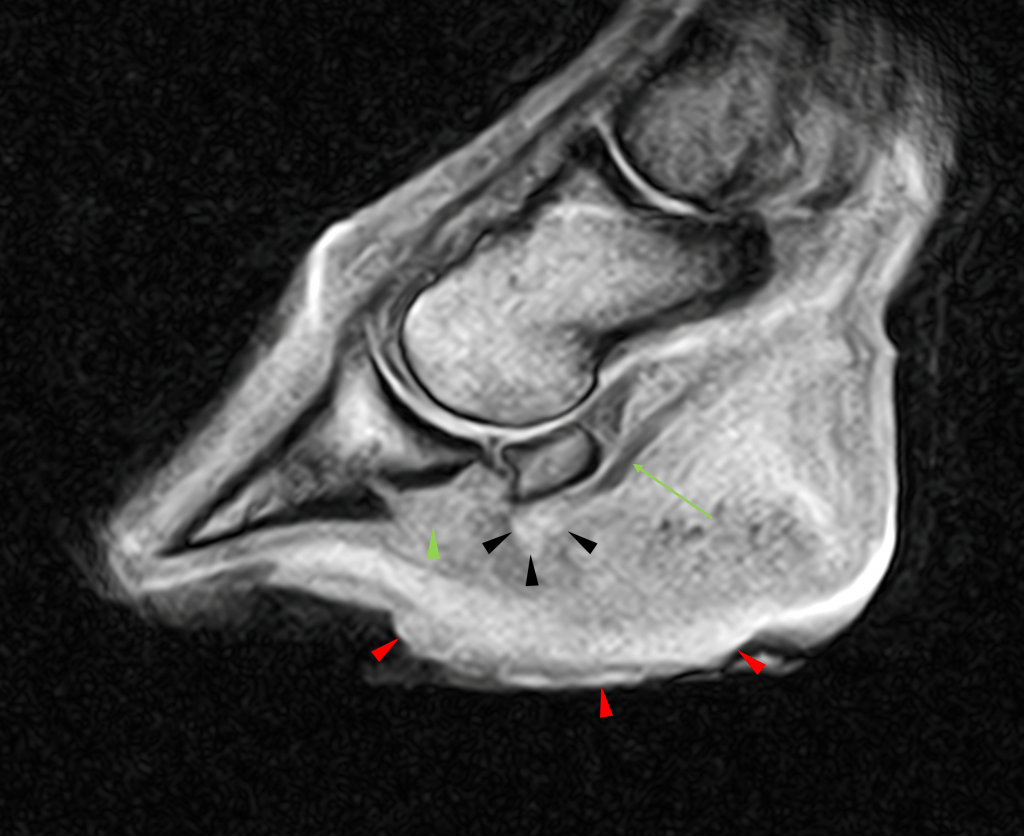
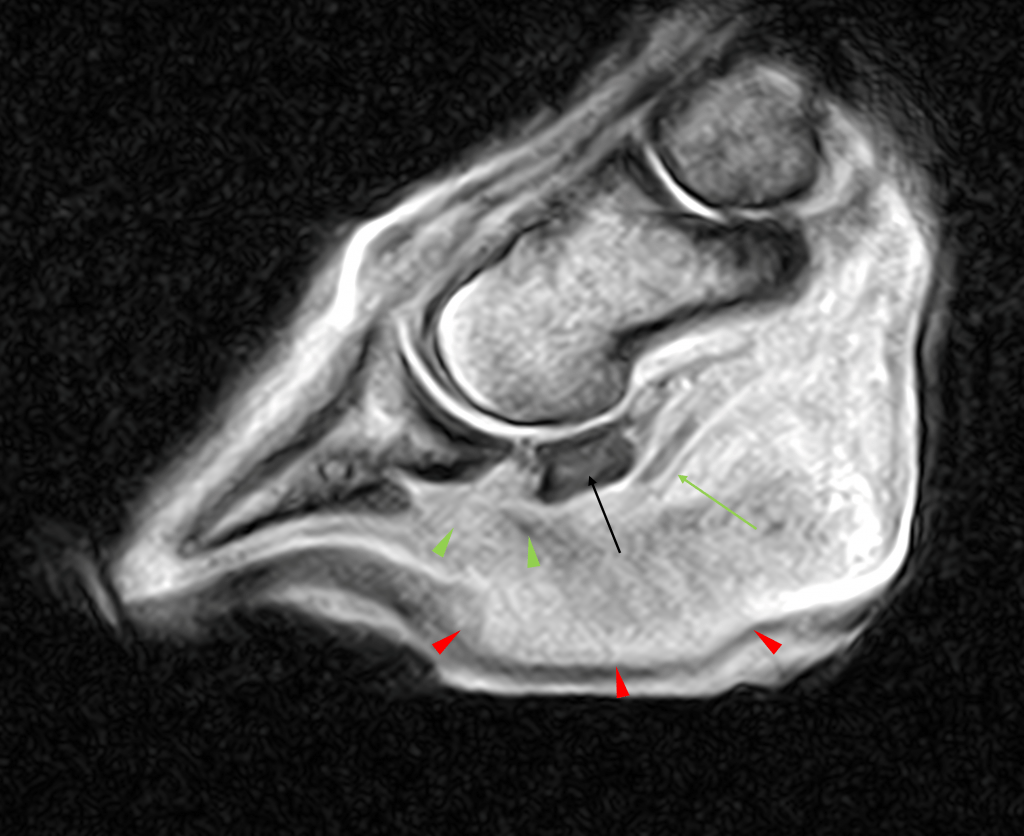
A more normal contour to the solar tissues(red arrowheads) was seen on the T1 sagittal images (previous scan to the left, recent to the right). The solar dermis was still disrupted although some organisation was evident. The green arrowheads show the persistent loss to the deep digital flexor tendon (DDFT) whilst there was a greater fluid signal within the navicular bone (black arrow).

Encouragingly the DDFT had not degenerated further. However, there was concern about the bone margins and increase in fluid signal within the distal phalanx and navicular bone. This, alongside the poor resolution of the bone margins, made the potential for osteolysis/osteonecrosis/osteomyelitis an increasing possibility for the mare.
Conclusions
- Loss of architecture to the lateral distal part of the DDFT although this was not more extensive than the previous study.
- The draining tract and granulation tissue had reduced in size, with an increase in dermal organisation
- Osteomyelitis remained a concern
- The navicular bursa remained distended
Case 4 – MRI Findings
Encouragingly, there was a reduction in fluid signal in the deep digital flexor tendon as shown on the below STIR frontal images (previous study to the left and recent to the right).
There was partial resolution of the fluid signal in the solar tissues (red arrowheads) and decreasing signal within the lateral aspect of the DDFT (red arrows) on the T2 FSE transverse image (previous to the left and recent to the right).
The tract had reduced in size further, with increased organisation within the dermis.
The interosseous signal pattern remained largely static. The clinical picture along with these findings made an osteonecrotic process less likely.
Conclusions
- The margins of the DDFT were becoming more clearly demarcated.
- The draining tract and granulation tissue continued to reduce in size.
- Osteomyelitis was less of a concern from the clinical presentation.
- The navicular bursa was less distended.
The mare went on to make a full recovery and is comfortable. She will continue her life as a broodmare. The referring clinician for this case puts her recovery down to the performed imaging and careful consideration of her clinical findings in light of the radiographic reports.