


Hyperextension of right front metacarpophalangeal joint
History
An 8-week-old Hanoverian mare foal was born with hyperextension of the right front metacarpophalangeal joint and treated conservatively using heavy distal limb bandaging and walking on a hard surface for 5 mins, three times daily. The foal showed mild colic symptoms, therefore it was placed in a small paddock, where it ran and jumped around. The next day, the foal showed 3-4/5 right front lameness with moderate swelling in the fetlock region. The foal received anti-inflammatories (meloxicam 0.6/kg P.O), muscle relaxant (methocarbamol 15–20 mg/kg) SID P.O and paraffin oil (13mL P.O SID).
Clinical examination
Upon presentation, the foal was alert and all vital parameters were within normal limits. The right front fetlock region showed moderate soft tissue swelling, more obviously on the lateral aspect. No lameness could be seen at walk. At trot, on hard surface, mild to moderate (2-3/5) right front lameness was observed.
Radiography findings
Dorso-palmar (DP) and dorsomedial15-25° palmaro-medial radiographs were reviewed (carried out by the referring vet). Radiography showed that the lateral proximal sesamoid bone (SB) is dislocated in a proximal and abaxial direction from its normal anatomical location (Fig. 1a). The long axis of the lateral SB is rotated clockwise approximately 45° to the long axis of the limb (Fig. 1b). The shape and the bone density of the lateral SB were unremarkable. Moderate soft tissue swelling on the lateral aspect of the fetlock can be seen.


CT findings
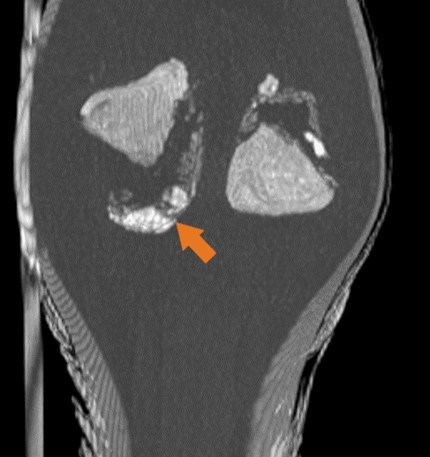
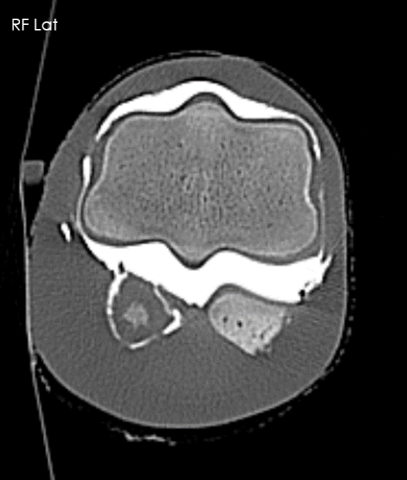
CT (Multi-slice Aquilion LB) was performed to obtain further information regarding the surrounding soft tissue and for surgical planning. CT was carried under heavy sedation xylazine (0.8mg/Kg i.v.) in right lateral recumbency. The CT revealed displacement of the lateral sesamoid bone (SB). There is moderate heterogeneous dystrophic mineralization in the normal anatomical region of the displaced SB. The lateral suspensory branch as well as the lateral oblique sesamoidean ligament were intact. The medial SB showed mild heterogeneous dystrophic mineralization at the apical region with mild disruption of the ipsilateral suspensory branch. There is also mild to moderate distention of the metacarpophalangeal joint. The flexor tendons are slightly displaced medially.
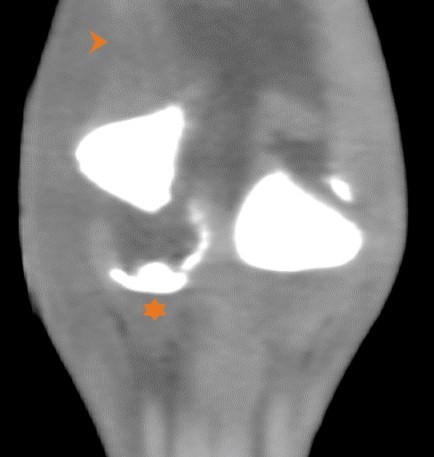
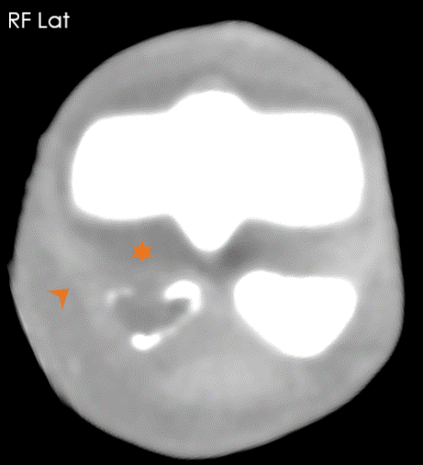
The lateral proximal sesamoid bone is dislocated proximally and abaxially (Fig. 2a). There is heterogenic bone attenuation material at the distal and axial border of the normal anatomical location of the sesamoid bone (arrow). The insertional region of the lateral suspensory branch is unremarkable (Fig. 2b) however, the suspensory branch showed slightly hypo attenuated region in the middle third, which is more likely to be an artefact due to relaxation of the fibres (arrow-head). The distal sesamoid ligaments were unremarkable and inserted in the bony material at the normal anatomical region of the lateral proximal sesamoid ligament (star).
3 palmar 3D view (A) of the right front fetlock showing the proximal sesamoid bones (Fig. 2c). There is irregular thickened mineralization at the base of the normal anatomical location of the lateral proximal sesamoid bone (Fig. 2d). The lateral collateral sesamoid ligament is mildly thickened and inserted in the mineralization region (arrow). There is also mild dislocation of the flexor tendons medially and mild distension of the palmar process of the metacarpophalangeal joint (star).

Diagnosis
Traumatic rupture of the suspensory apparatus.
Treatment options
Surgical intervention would be required, aiming to reposition the lateral sesamoid bone to its normal anatomical position and maintain normal positioning through internal fixation with the medial sesamoid bone. Based on the difficulty of the surgery and poor prognosis, the owner elected euthanasia. MRI was subsequently performed postmortem.
Post Mortem MRI findings
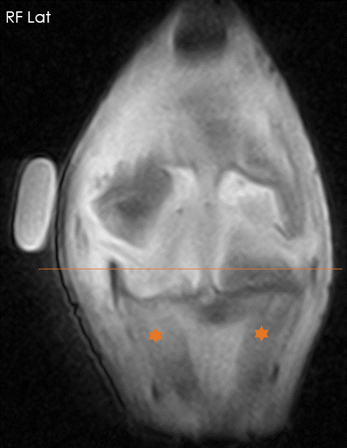
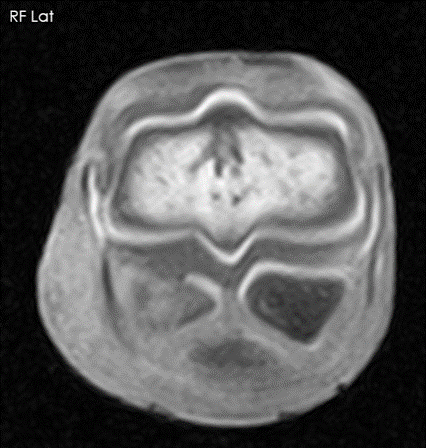
MRI (using the Hallmarq 0.27T magnet) was performed and revealed normal shape, size and signal intensity of both proximal sesamoid bones. The space left by the displaced lateral BS showed moderate-high signal intensity, surrounded by a cartilage-like structure in all image sequences. There is a moderate pooling of the synovial fluid from the joint (Fig. 5), indicating a tear of the palmar recess of the fetlock. The lateral collateral sesamoid ligament as well as the sesamoidean ligaments were well defined and intact. Interestingly, that the sesamoidean ligaments insert on the cartilaginous like structure. The insertion of the proximal annular ligament showed mild to moderate thickening with moderate high signal intensity. Based on the MRI finding, CT arthrography of the metacarpophalangeal joint was carried out to confirm the tear of the palmar recess of the joint.
The oblique ligaments (Fig. 3a stars) as well as the inter sesamoid ligaments are intact and inserted at their physiological region in spite dislocation of the lateral proximal sesamoid bone (Fig. 3a). There is discontinuation of the cartilaginous layer at the dorsal aspect of the anatomical location of the lateral sesamoid ligament.
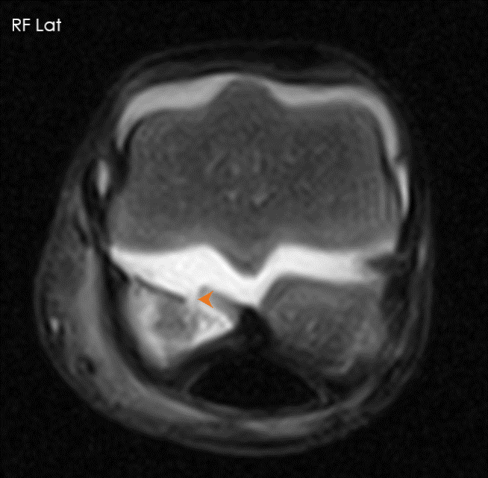
There is a synovial fluid extending from the palmar recess of the fetlock (Fig. 3c arrow-head) and pooling at the anatomical location of the lateral sesamoid bone. This finding has been confirmed using a contrast arthrography. The contrast has pooled around the anatomical region of the sesamoid bone (Fig. 3d).
Discussion
Proximal dislocation of the proximal sesamoid bone without fracture can occur with traumatic rupture of the distal sesamoidean ligaments. Besides the severe trauma sustained to the supporting soft tissues and bone, the adjacent digital arteries are frequently damaged sufficiently to result in ischemic necrosis of the hoof (Miller and Juzwiak, 2010).
Extreme overextension of the fetlock is the other likely cause for disruption of the suspensory apparatus, more frequently seen in racehorses.
The MRI of the current foal showed that the soft tissues of the suspensory apparatus were intact, in particular the oblique, straight and straight sesamoid ligaments. Such lesions have rarely been documented in foals. Honnas et al. (1990) reported traumatic rupture of the suspensory apparatus in three foals. All three foals had been diagnosed with a fracture of the sesamoid bones. In this case, sesamoid bones were intact.
Interestingly, the dislocated sesamoid bone was surrounded with synovial fluid from the joint, which complicated the potential surgical intervention. The foals from Honnas et al. (1990) were treated with limb casting for 4 weeks and followed up for a 2-year period. One foal was euthanized and two foals had favorable outcomes 2-3 years post-treatment.
Conclusion
In this case, the MRI was superior in diagnosis of the soft tissue and synovial tear compared to plain CT. However, contrast arthrography provided morphological information regarding the synovial tear. The combination of the two imaging modalities provided more details and greater understanding of the pathology in this interesting and unusual case.
With thanks to Tierklinik Lüshce for providing this case study.
