

A left hind limb lameness resulting from a thrombosed digital artery
History
A 6-year-old Irish sports horse presented with a history of grade 3/5 left hind lameness. The lameness had improved following an abaxial sesamoid nerve block. Radiographs taken by the referring vet revealed an abnormal lucency in the distal phalanx and MRI was recommended for further investigation.
MRI Findings
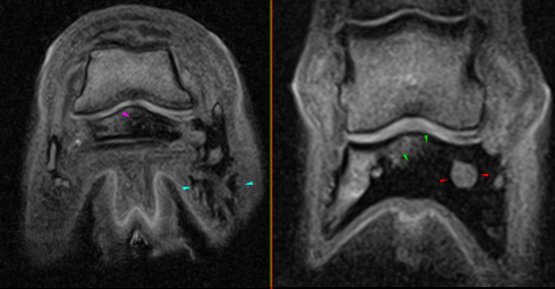
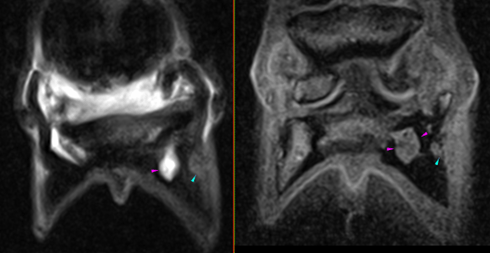
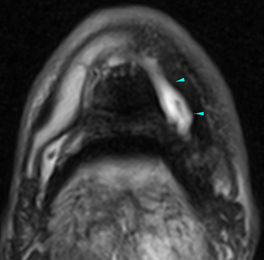
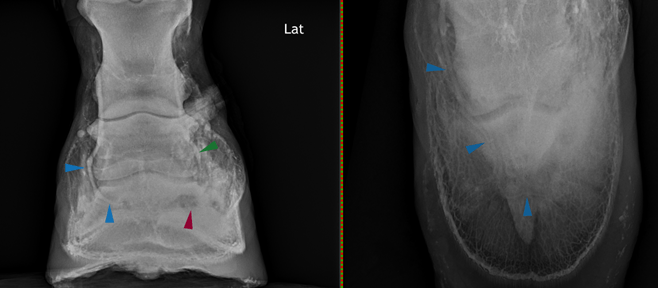
- Marked dilatation of the lateral vessels of the distal phalanx with surrounding fluid signal and sclerosis of the lateral half of the distal phalanx as well as marked thickening of the lateral plantar process, with aberrant vascular channels within this. The fluid signal within the bone may indicate that active modelling is ongoing
- Mild to moderate fluid signal within the navicular bone, likely consistent with altered loading of the bone
- Moderate distal interphalangeal joint effusion, which is a non-specific sign and may be secondary to other inflammation within the foot
- Mild distal interphalangeal joint osteoarthropathy
Differential diagnoses for dilated vasculature
- Marked chronic pedal osteitis, with possible thrombosis and secondary dilatation of the vascular channels
- Aneurysm of the lateral half of the proper plantar digital artery, with formation of collateral circulation
- An aneurysmal bone cyst (less likely)
Given the thickening of the lateral plantar process and the suspected aberrant vascular channels, it was decided to proceed to a CT examination of the foot, to give greater osseous detail and delineate the suspected aberrant vascular channels.
CT Findings
CT examination confirmed the dilation of the vascular channels of the lateral half of the distal phalanx, with a prominent laterally located channel, which was thought to represent collateral circulation.
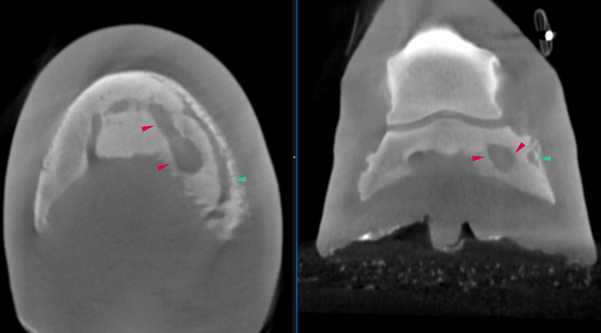
The cause of the marked dilatation of the lateral portion of the terminal arch was not established. CT angiography was discussed, however, this was not possible. Positive contrast venography was carried out, which revealed filling defects in the lateral proper plantar digital artery, extending from the midpoint of the terminal arch to the mid diaphysis of the middle phalanx. There remained good contrast filling of the remainder of the lateral vasculature, likely indicating adequate collateral circulation.
Conclusions
The patient was diagnosed with thrombosis of the lateral proper digital artery with dilatation portion of the terminal arch, which was presumed to be due to pressure necrosis secondary to enlargement of the vasculature.
The MRI and CT showed that the unusual lucency detected radiographically within the distal phalanx represented the lateral portion of the terminal arch. MRI examination showed fluid signal within the bone surrounding this, likely indicating osseous activity. The CT examination confirmed the dilatation of the terminal arch and highlighted the presence of a collateral vessel. The cause of the dilatation was confirmed as thrombosis using venography.
Scans were performed using Hallmarq’s Standing Equine MRI and Standing Equine Leg CT systems. Images and interpretation provided in collaboration with VetCT.


