


10-year-old Irish Sports horse with an inflammatory bone lesion in the pastern
History
Initially, the gelding was given 3 months pasture rest. On examination after this rest period, the horse was short striding when turning in a small circle to the left on a hard surface. Re-examination a few weeks later showed the gelding had progressed to exhibit LF lameness in canter and trot. Both left and right forelimb distal interphalangeal joints were medicated, and a further 25 days box/stall rest was advised.
Clinical examination
On re-examination, a 3/5 (AAEP lameness grade) left forelimb lameness was observed, which became more severe when the horse was lunged on the left rein in a small circle on the hard. An abaxial sesamoid nerve block abolished the left forelimb lameness and elicited a mild (deemed to be non-relevant) right forelimb lameness. DIP joint analgesia of the left forelimb elicited a 60% positive response.
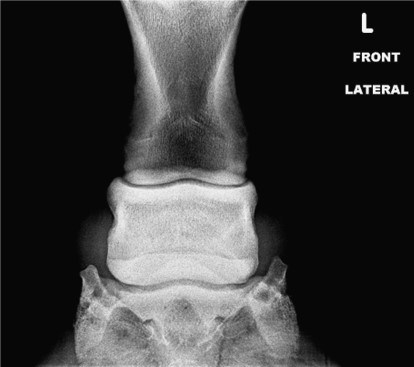
Radiography findings
The radiographs were unremarkable; no clinically relevant abnormalities were noted (figures 1 and 2). Due to the severity of lameness and lack of findings on radiography, MRI was performed.

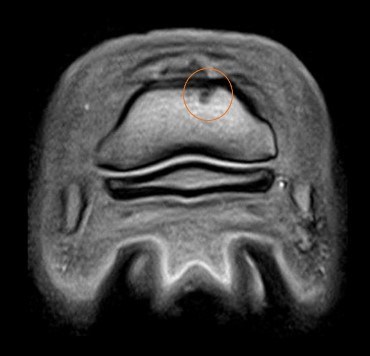
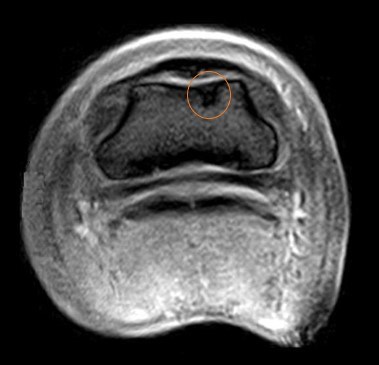
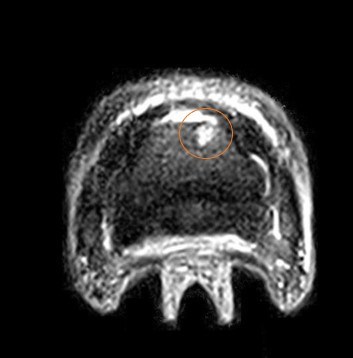
MRI findings
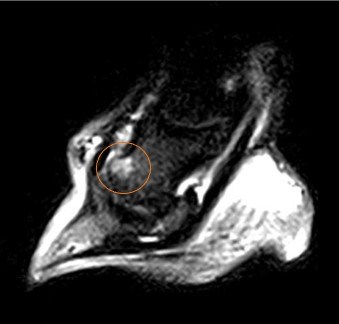
A focal, irregular area of decreased signal on both T1 and T2* weighted images (figure 3 and 4) at the distal dorsal aspect of the middle phalanx just lateral to the sagittal midline. This was adjacent to the dorsal articular cartilage but did not appear to involve the joint. The lesion produced high signal in the STIR sequences, indicative of excessive fluid presence within the bone (figure 5).

Conclusion and diagnosis
The MRI findings indicated an inflammatory lesion within the bone of the dorsal distal aspect of the middle phalanx. Differential diagnoses included; oedema, necrosis, infection, ischemia or a cystic like bone lesion. Re-examination with MRI 8 weeks later revealed no abnormalities indicating the lesion had resolved and increasing the likelihood of traumatic origin.
Diagnosis: Focal middle phalanx bone inflammation.
Treatment and prognosis
Initially, the horse was pasture rested for 5 months. The horse was then slowly brought back into work. Walking work only was recommended for the first 6 weeks and then reassessment before progressing with rehabilitation. Unfortunately, reassessment at 6 weeks revealed only minor improvement in the lameness and a decision was made to retire the horse from show jumping.


